

A Framework For Step Down Or Therapeutic Re-Organization For Withdrawal Of Inhaled Corticosteroids In Selected Patients With COPD: A Proposal For COPD Management
- PMID: 31576115
- PMCID: PMC6765263
- DOI: 10.2147/COPD.S216059
A Framework For Step Down Or Therapeutic Re-Organization For Withdrawal Of Inhaled Corticosteroids In Selected Patients With COPD: A Proposal For COPD Management
Abstract
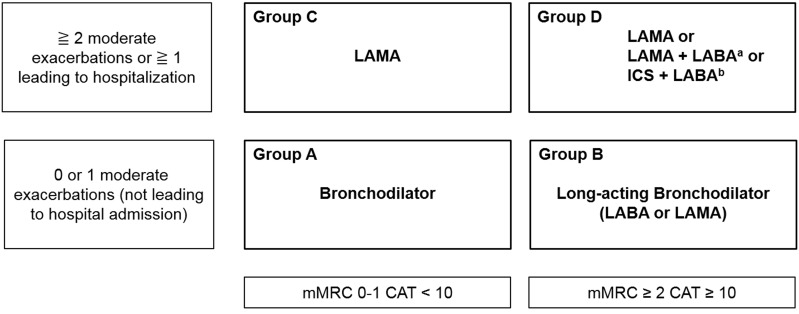
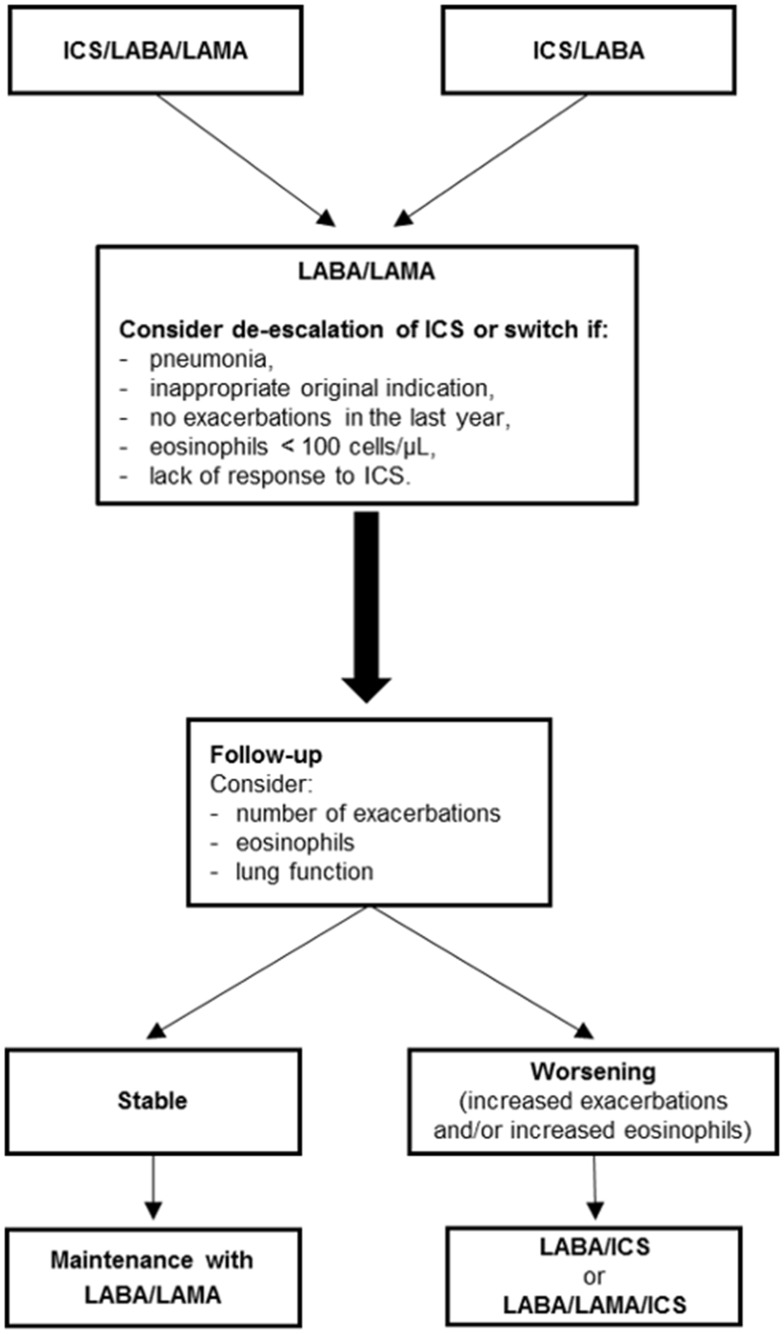
While chronic obstructive pulmonary disease (COPD) continues to be a major cause of morbidity and mortality, pharmacological therapy has a definite benefit on symptoms as well as the frequency and severity of exacerbations, and general health. The most recent Global Initiative for Obstructive Lung Disease (GOLD) guidelines recommend triple therapy (long-acting beta2 agonists [LABA] + long-acting muscarinic antagonists [LAMA] + inhaled corticosteroids [ICS]) only for patients with exacerbations, elevated eosinophils, and without control using a LABA/LAMA or ICS/LABA combination. Long-term monotherapy with ICS is not currently recommended, but may be considered in association with LABAs in patients with a history of exacerbations and elevated eosinophils in spite of appropriate treatment with long-acting bronchodilators. However, long-term use of ICS in combination therapy has been associated with adverse effects, even if widely used in routine management for decades. The available evidence suggests that ICS can be rationally discontinued in patients with stable disease and is not likely to have unfavorable effects on lung function, overall health, or be associated with a greater risk of exacerbations. Indeed, it is widely accepted that ICS therapy should be limited to a small proportion of patients after careful assessment of the individual risk-benefit profile. Unfortunately, however, there are no international recommendations that provide specific guidance or a protocol for withdrawal of ICS. Herein, the available evidence on the use of ICS is reviewed and an easy to use tool is proposed that can provide clinicians with a simple management scheme to guide the most appropriate therapy for management of COPD and use of ICS. In management of COPD, a highly personalized approach is advocated so that the most appropriate therapy for each individual patient can be selected.
Keywords: COPD; LABA; LAMA; deprescribing; exacerbation; inhaled corticosteroids.
© 2019 Micheletto et al.
Conflict of interest statement
Claudio Micheletto reports personal fees from AstraZeneca, GSK, Menarini, Guidotti, Berlin Chemie, Novartis, Zambom, and Boehringer Ingelheim, outside the submitted work. Marco Contoli reports grants and personal fees from AstraZeneca and Chiesi, and personal fees from ALK-Abello, Novartis, Zambon, GlaxoSmithKline, and Boehringer Ingelheim, outside the submitted work. Fabiano Di Marco reports grants, personal fees, and non-financial support from AstraZeneca, Boehringer Ingelheim, Chiesi, Novartis, Menarini, Malesci, Guidotti, TEVA, and Zambon, outside the submitted work. Pierachille Santus reports grants and personal fees from Boehringer Ingelheim and AstraZeneca, grants from Chiesi Farmaceutici and Almirall, and personal fees from ALK-Abello, Berlin Chemie, GSK, Sanofi, and Zambon Italia, during the conduct of the study. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
Stepwise management of COPD: What is next after bronchodilation?Ther Adv Respir Dis. 2023 Jan-Dec;17:17534666231208630. doi: 10.1177/17534666231208630. Ther Adv Respir Dis. 2023. PMID: 37936381 Free PMC article. Review.
-
Current evidence for COPD management with dual long-acting muscarinic antagonist/long-acting β2-agonist bronchodilators.Postgrad Med. 2020 Mar;132(2):198-205. doi: 10.1080/00325481.2019.1702834. Epub 2020 Jan 3. Postgrad Med. 2020. PMID: 31900019 Review.
-
Comparative Effectiveness of Long-Acting Beta2 -Agonist Combined with a Long-Acting Muscarinic Antagonist or Inhaled Corticosteroid in Chronic Obstructive Pulmonary Disease.Pharmacotherapy. 2017 Apr;37(4):447-455. doi: 10.1002/phar.1913. Pharmacotherapy. 2017. PMID: 28226405
-
Role of Long-Acting Muscarinic Antagonist/Long-Acting β2-Agonist Therapy in Chronic Obstructive Pulmonary Disease.Ann Pharmacother. 2017 Aug;51(8):696-705. doi: 10.1177/1060028017705149. Epub 2017 Apr 14. Ann Pharmacother. 2017. PMID: 28410560 Review.
-
Inhaled Corticosteroid Treatment in Chronic Obstructive Pulmonary Disease (COPD): Boon or Bane?J Am Board Fam Med. 2020 Mar-Apr;33(2):289-302. doi: 10.3122/jabfm.2020.02.190227. J Am Board Fam Med. 2020. PMID: 32179613 Review.
Cited by
-
Withdrawal of inhaled corticosteroids versus continuation of triple therapy in patients with COPD in real life: observational comparative effectiveness study.Respir Res. 2021 Jan 21;22(1):25. doi: 10.1186/s12931-021-01615-0. Respir Res. 2021. PMID: 33478491 Free PMC article.
-
Clinical and Economic Impact of Long-Term Inhaled Corticosteroid Withdrawal in Patients with Chronic Obstructive Pulmonary Disease Treated with Triple Therapy in Spain.Int J Chron Obstruct Pulmon Dis. 2022 Sep 7;17:2161-2174. doi: 10.2147/COPD.S367708. eCollection 2022. Int J Chron Obstruct Pulmon Dis. 2022. PMID: 36101793 Free PMC article.
References
-
- Global initiative for chronic obstructive lung disease (GOLD) 2019 report. Available from: https://goldcopd.org/gold-reports/. Accessed September10, 2019.
