

Characteristic Pattern of IL-17RA, IL-17RB, and IL-17RC in Monocytes/Macrophages and Mast Cells From Patients With Bullous Pemphigoid
- PMID: 31572359
- PMCID: PMC6749098
- DOI: 10.3389/fimmu.2019.02107
Characteristic Pattern of IL-17RA, IL-17RB, and IL-17RC in Monocytes/Macrophages and Mast Cells From Patients With Bullous Pemphigoid
Abstract
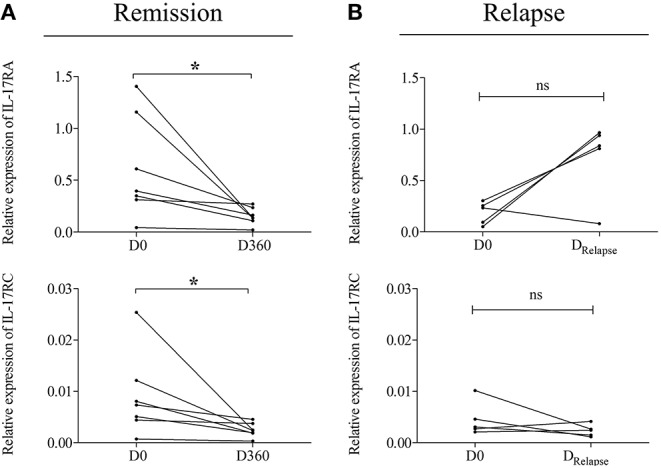
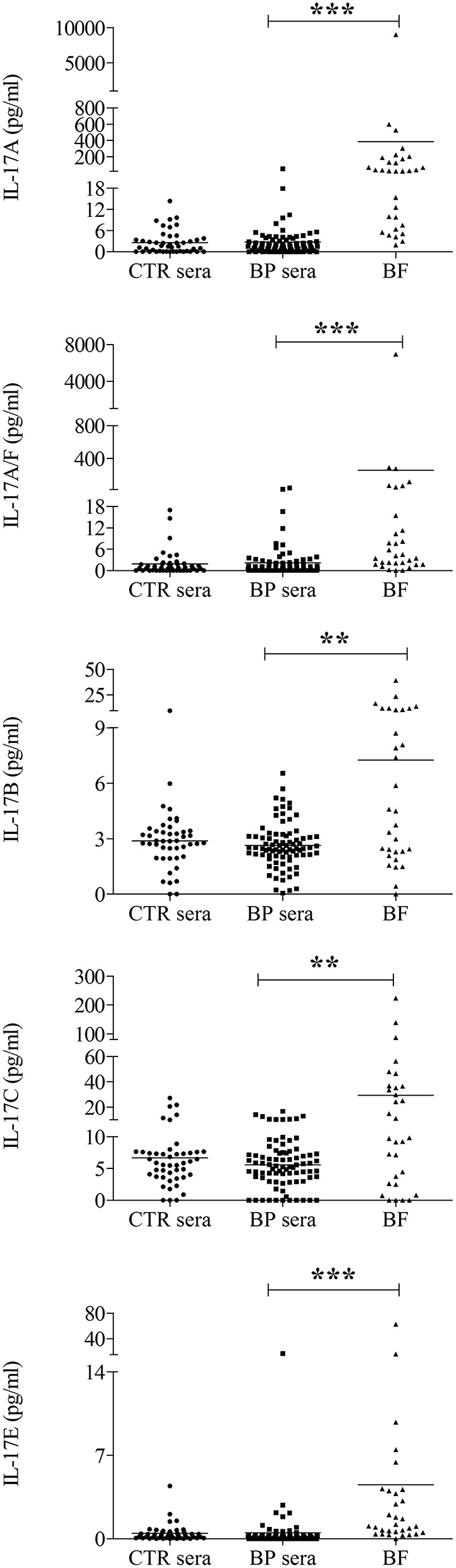
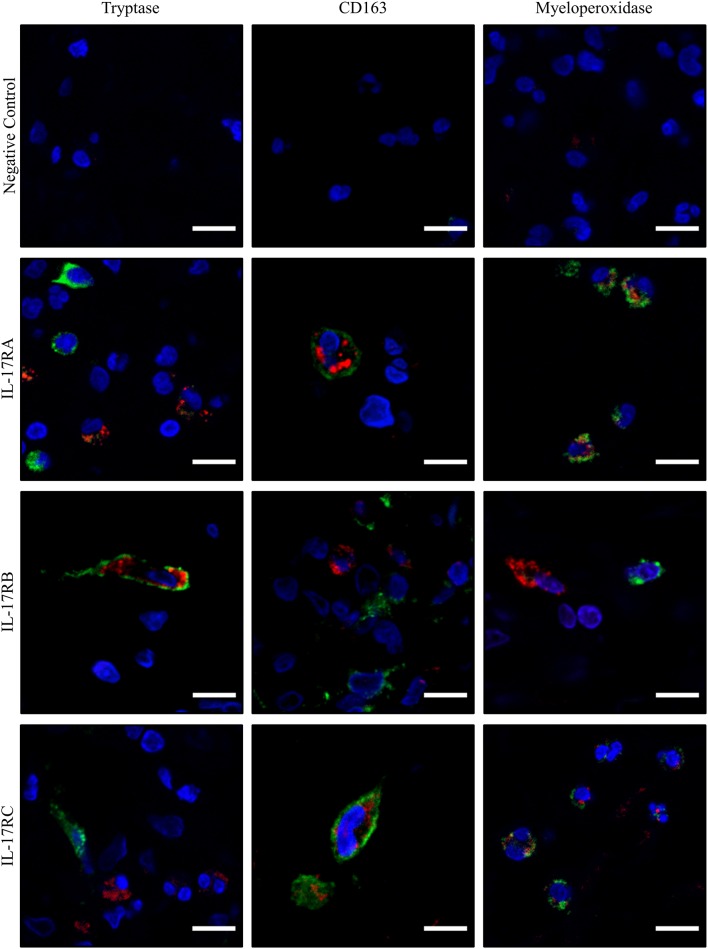
Inflammation is largely implicated in bullous pemphigoid (BP), the most frequent skin auto-immune blistering disease. IL-17, essentially IL-17A/F, has been involved in blister formation through regulation of protease production, and its specific serum profile within BP was related to disease outcome. However, relationships between IL-17 family ligands and receptors are quite complex with six different IL-17 isoforms, and five different receptors. We here aimed at clarifying the contribution of the IL-17 axis in BP by characterizing not only the expression of IL-17 receptor (IL-17R) members within immune cells isolated from BP patients (PMNs, n = 9; T-lymphocytes, n = 10; and monocytes, n = 10) but also the expression of IL-17 isoforms in sera (n = 83), and blister fluid (n = 31) of BP patients. We showed that at diagnosis, IL-17RA and IL-17RC expression were significantly increased in monocytes isolated from BP patients as compared to those from control subjects (p = 0.006 and p = 0.016, respectively). Notably, both IL-17RA and IL-17RC mRNA expression remained elevated in BP monocytes at time of relapse. We further demonstrated a significant increase of all IL-17 isoforms tested in BP blister fluid compared with BP serum (IL-17A, p < 0.0001; IL-17A/F, p < 0.0001; IL-17B, p = 0.0023; IL-17C, p = 0.0022; IL-17E, p < 0.0001). Among all, IL-17B was the only cytokine for which a significant decreased concentration within blister fluid was observed in BP patients with severe disease compared to patients with moderate disease (p = 0.012). We further evidenced a significant negative correlation between IL-17B levels and blister/erosion BPDAI subscore (r = -0.52, p = 0.003). We finally identified mast cells as a potential target of IL-17B in lesional skin of BP patients. In conclusion, we showed here that IL-17RA and IL-17RC expression in monocyte was associated with disease activity and evidenced in situ a negative correlation between BP disease activity and IL-17B, whose effects could be mediated by IL-17RB expressed by mast cell in BP lesional skin.
Keywords: IL-17 isoforms; IL-17 receptors; autoimmunity; bullous pemphigoid; inflammation.
Copyright © 2019 Nesmond, Muller, Le Naour, Viguier, Bernard, Antonicelli and Le Jan.
Figures


Similar articles
-
Bullous pemphigoid outcome is associated with CXCL10-induced matrix metalloproteinase 9 secretion from monocytes and neutrophils but not lymphocytes.J Allergy Clin Immunol. 2017 Mar;139(3):863-872.e3. doi: 10.1016/j.jaci.2016.08.012. Epub 2016 Sep 13. J Allergy Clin Immunol. 2017. PMID: 27637385
-
Blister Fluid Induces MMP-9-Associated M2-Type Macrophages in Bullous Pemphigoid.Front Immunol. 2019 Aug 7;10:1858. doi: 10.3389/fimmu.2019.01858. eCollection 2019. Front Immunol. 2019. PMID: 31440247 Free PMC article.
-
Characterization of the interleukin-17 isoforms and receptors in lesional psoriatic skin.Br J Dermatol. 2009 Feb;160(2):319-24. doi: 10.1111/j.1365-2133.2008.08902.x. Epub 2008 Oct 21. Br J Dermatol. 2009. PMID: 19016708
-
The Autoimmune Skin Disease Bullous Pemphigoid: The Role of Mast Cells in Autoantibody-Induced Tissue Injury.Front Immunol. 2018 Mar 1;9:407. doi: 10.3389/fimmu.2018.00407. eCollection 2018. Front Immunol. 2018. PMID: 29545809 Free PMC article. Review.
-
IL-17RC: a partner in IL-17 signaling and beyond.Semin Immunopathol. 2010 Mar;32(1):33-42. doi: 10.1007/s00281-009-0185-0. Epub 2009 Dec 13. Semin Immunopathol. 2010. PMID: 20012905 Free PMC article. Review.
Cited by
-
The IL-23/IL-17 Pathway in Inflammatory Skin Diseases: From Bench to Bedside.Front Immunol. 2020 Nov 17;11:594735. doi: 10.3389/fimmu.2020.594735. eCollection 2020. Front Immunol. 2020. PMID: 33281823 Free PMC article. Review.
-
IL-17A Increases Doxorubicin Efficacy in Triple Negative Breast Cancer.Front Oncol. 2022 Jul 18;12:928474. doi: 10.3389/fonc.2022.928474. eCollection 2022. Front Oncol. 2022. PMID: 35924165 Free PMC article.
-
SARS-CoV-2 ORF8 Mediates Signals in Macrophages and Monocytes through MyD88 Independently of the IL-17 Receptor.J Immunol. 2023 Jul 15;211(2):252-260. doi: 10.4049/jimmunol.2300110. J Immunol. 2023. PMID: 37265402 Free PMC article.
-
Serum Biomarkers in Bullous Pemphigoid: A Systematic Review.J Cutan Med Surg. 2024 Sep-Oct;28(5):463-467. doi: 10.1177/12034754241266171. Epub 2024 Jul 29. J Cutan Med Surg. 2024. PMID: 39075716 Free PMC article.
-
Propionic acid ameliorates cognitive function through immunomodulatory effects on Th17 cells in perioperative neurocognitive disorders.Heliyon. 2024 Mar 27;10(8):e28817. doi: 10.1016/j.heliyon.2024.e28817. eCollection 2024 Apr 30. Heliyon. 2024. PMID: 38699705 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials