

The Immune Landscape of Thyroid Cancer in the Context of Immune Checkpoint Inhibition
- PMID: 31412566
- PMCID: PMC6720642
- DOI: 10.3390/ijms20163934
The Immune Landscape of Thyroid Cancer in the Context of Immune Checkpoint Inhibition
Abstract
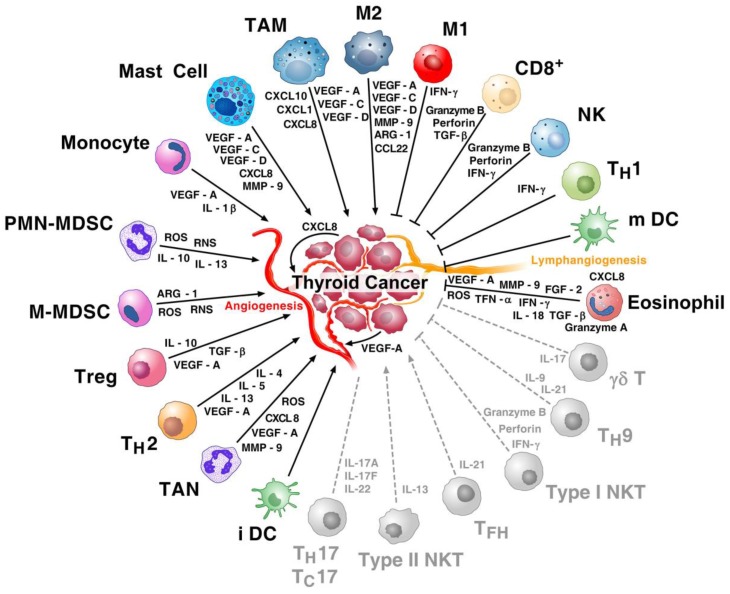
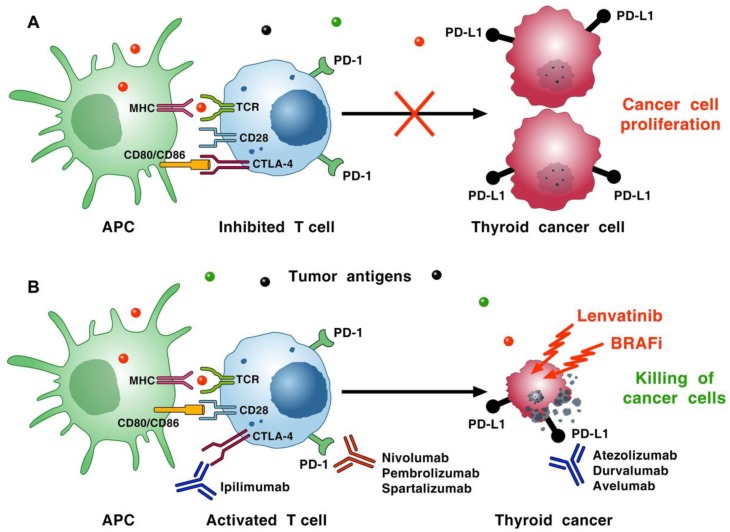
Immune cells play critical roles in tumor prevention as well as initiation and progression. However, immune-resistant cancer cells can evade the immune system and proceed to form tumors. The normal microenvironment (immune cells, fibroblasts, blood and lymphatic vessels, and interstitial extracellular matrix (ECM)) maintains tissue homeostasis and prevents tumor initiation. Inflammatory mediators, reactive oxygen species, cytokines, and chemokines from an altered microenvironment promote tumor growth. During the last decade, thyroid cancer, the most frequent cancer of the endocrine system, has emerged as the fifth most incident cancer in the United States (USA), and its incidence is steadily growing. Inflammation has long been associated with thyroid cancer, raising critical questions about the role of immune cells in its pathogenesis. A plethora of immune cells and their mediators are present in the thyroid cancer ecosystem. Monoclonal antibodies (mAbs) targeting immune checkpoints, such as mAbs anti-cytotoxic T lymphocyte antigen 4 (anti-CTLA-4) and anti-programmed cell death protein-1/programmed cell death ligand-1 (anti-PD-1/PD-L1), have revolutionized the treatment of many malignancies, but they induce thyroid dysfunction in up to 10% of patients, presumably by enhancing autoimmunity. Combination strategies involving immune checkpoint inhibitors (ICIs) with tyrosine kinase (TK) or serine/threonine protein kinase B-raf (BRAF) inhibitors are showing considerable promise in the treatment of advanced thyroid cancer. This review illustrates how different immune cells contribute to thyroid cancer development and the rationale for the antitumor effects of ICIs in combination with BRAF/TK inhibitors.
Keywords: CXCL8; T reg cells; angiogenesis; chemokines; dendritic cells; lymphangiogenesis; macrophages; mast cells; neutrophils; thyroid cancer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Immune Checkpoint Inhibition for Pancreatic Ductal Adenocarcinoma: Current Limitations and Future Options.Front Immunol. 2018 Aug 15;9:1878. doi: 10.3389/fimmu.2018.01878. eCollection 2018. Front Immunol. 2018. PMID: 30158932 Free PMC article. Review.
-
Tumor matrix remodeling and novel immunotherapies: the promise of matrix-derived immune biomarkers.J Immunother Cancer. 2018 Jul 3;6(1):65. doi: 10.1186/s40425-018-0376-0. J Immunother Cancer. 2018. PMID: 29970158 Free PMC article. Review.
-
Immune checkpoint inhibitors: The linchpins of modern immunotherapy.Immunol Rev. 2019 Jul;290(1):6-23. doi: 10.1111/imr.12766. Immunol Rev. 2019. PMID: 31355494 Review.
-
Angiopoietin-2 as a Biomarker and Target for Immune Checkpoint Therapy.Cancer Immunol Res. 2017 Jan;5(1):17-28. doi: 10.1158/2326-6066.CIR-16-0206. Epub 2016 Dec 21. Cancer Immunol Res. 2017. PMID: 28003187 Free PMC article.
-
Overcoming Resistance to Combination Radiation-Immunotherapy: A Focus on Contributing Pathways Within the Tumor Microenvironment.Front Immunol. 2019 Jan 31;9:3154. doi: 10.3389/fimmu.2018.03154. eCollection 2018. Front Immunol. 2019. PMID: 30766539 Free PMC article. Review.
Cited by
-
The role of immune cells and immune related genes in the tumor microenvironment of papillary thyroid cancer and their significance for immunotherapy.Sci Rep. 2024 Aug 5;14(1):18125. doi: 10.1038/s41598-024-69187-9. Sci Rep. 2024. PMID: 39103463 Free PMC article.
-
Targeting SHP2 sensitizes differentiated thyroid carcinoma to the MEK inhibitor.Am J Cancer Res. 2022 Jan 15;12(1):247-264. eCollection 2022. Am J Cancer Res. 2022. PMID: 35141016 Free PMC article.
-
Mutations in lysine methyltransferase 2C and PEG3 are associated with tumor mutation burden, prognosis, and antitumor immunity in pancreatic adenocarcinoma patients.Digit Health. 2022 Oct 20;8:20552076221133699. doi: 10.1177/20552076221133699. eCollection 2022 Jan-Dec. Digit Health. 2022. PMID: 36312851 Free PMC article.
-
Comprehensive analysis of BTNL9 as a prognostic biomarker correlated with immune infiltrations in thyroid cancer.BMC Med Genomics. 2023 Oct 5;16(1):234. doi: 10.1186/s12920-023-01676-8. BMC Med Genomics. 2023. PMID: 37798795 Free PMC article.
-
Cell and Molecular Biology of Thyroid Disorders 2.0.Int J Mol Sci. 2021 Feb 17;22(4):1990. doi: 10.3390/ijms22041990. Int J Mol Sci. 2021. PMID: 33671462 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
