

A qPCR expression assay of IFI44L gene differentiates viral from bacterial infections in febrile children
- PMID: 31409879
- PMCID: PMC6692396
- DOI: 10.1038/s41598-019-48162-9
A qPCR expression assay of IFI44L gene differentiates viral from bacterial infections in febrile children
Abstract
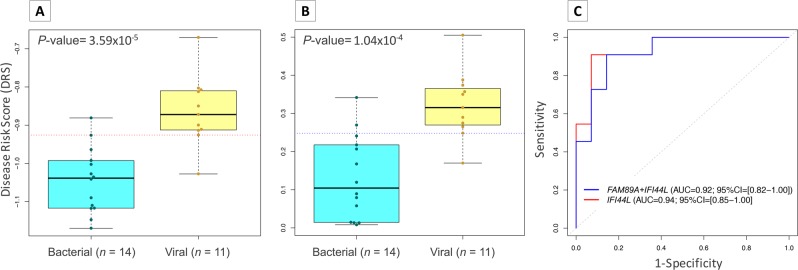
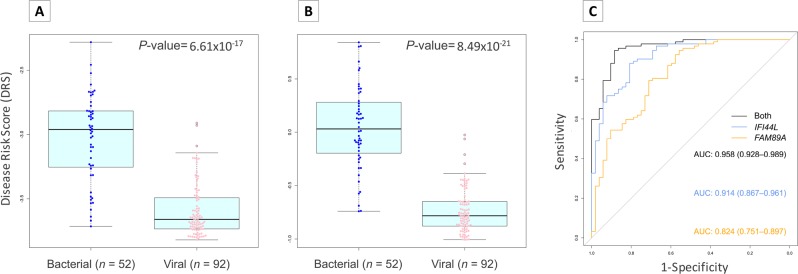
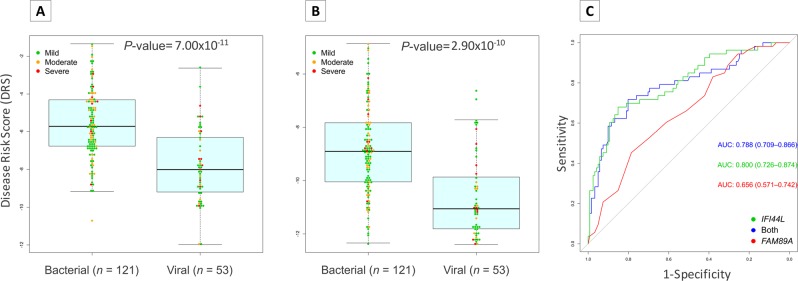
The diagnosis of bacterial infections in hospital settings is currently performed using bacterial culture from sterile site, but they are lengthy and limited. Transcriptomic biomarkers are becoming promising tools for diagnosis with potential applicability in clinical settings. We evaluated a RT-qPCR assay for a 2-transcript host expression signature (FAM89A and IFI44L genes) inferred from microarray data that allow to differentiate between viral and bacterial infection in febrile children. This assay was able to discriminate viral from bacterial infections (P-value = 1.04 × 10-4; AUC = 92.2%; sensitivity = 90.9%; specificity = 85.7%) and showed very high reproducibility regardless of the reference gene(s) used to normalize the data. Unexpectedly, the monogenic IFI44L expression signature yielded better results than those obtained from the 2-transcript test (P-value = 3.59 × 10-5; AUC = 94.1%; sensitivity = 90.9%; specificity = 92.8%). We validated this IFI44L signature in previously published microarray and whole-transcriptome data from patients affected by different types of viral and bacterial infections, confirming that this gene alone differentiates between both groups, thus saving time, effort, and costs. Herein, we demonstrate that host expression microarray data can be successfully translated into a fast, highly accurate and relatively inexpensive in vitro assay that could be implemented in the clinical routine.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Diagnostic Test Accuracy of a 2-Transcript Host RNA Signature for Discriminating Bacterial vs Viral Infection in Febrile Children.JAMA. 2016 Aug 23-30;316(8):835-45. doi: 10.1001/jama.2016.11236. JAMA. 2016. PMID: 27552617 Free PMC article.
-
A two-transcript biomarker of host classifier genes for discrimination of bacterial from viral infection in acute febrile illness: a multicentre discovery and validation study.Lancet Digit Health. 2021 Aug;3(8):e507-e516. doi: 10.1016/S2589-7500(21)00102-3. Lancet Digit Health. 2021. PMID: 34325854
-
FAM89A and IFI44L for distinguishing between viral and bacterial infections in children with febrile illness.Pediatr Investig. 2021 Sep 22;5(3):195-202. doi: 10.1002/ped4.12295. eCollection 2021 Sep. Pediatr Investig. 2021. PMID: 34589675 Free PMC article.
-
Transcript host-RNA signatures to discriminate bacterial and viral infections in febrile children.Pediatr Res. 2022 Jan;91(2):454-463. doi: 10.1038/s41390-021-01890-z. Epub 2021 Dec 15. Pediatr Res. 2022. PMID: 34912024 Review.
-
Differential Markers of Bacterial and Viral Infections in Children for Point-of-Care Testing.Trends Mol Med. 2020 Dec;26(12):1118-1132. doi: 10.1016/j.molmed.2020.09.004. Epub 2020 Sep 29. Trends Mol Med. 2020. PMID: 33008730 Free PMC article. Review.
Cited by
-
The Feasibility of Host Transcriptome Profiling as a Diagnostic Tool for Microbial Etiology in Childhood Cancer Patients with Febrile Neutropenia.Int J Mol Sci. 2020 Jul 26;21(15):5305. doi: 10.3390/ijms21155305. Int J Mol Sci. 2020. PMID: 32722616 Free PMC article. Clinical Trial.
-
TIPICO X: report of the 10th interactive infectious disease workshop on infectious diseases and vaccines.Hum Vaccin Immunother. 2021 Mar 4;17(3):759-772. doi: 10.1080/21645515.2020.1788301. Epub 2020 Aug 5. Hum Vaccin Immunother. 2021. PMID: 32755474 Free PMC article.
-
Implications of Using Host Response-Based Molecular Diagnostics on the Management of Bacterial and Viral Infections: A Review.Front Med (Lausanne). 2022 Feb 3;9:805107. doi: 10.3389/fmed.2022.805107. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35186993 Free PMC article. Review.
-
Rapid and simple single-chamber nucleic acid detection system prepared through nature-inspired surface engineering.Theranostics. 2021 May 3;11(14):6735-6745. doi: 10.7150/thno.57153. eCollection 2021. Theranostics. 2021. PMID: 34093850 Free PMC article.
-
Uncovering hub genes in sepsis through bioinformatics analysis.Medicine (Baltimore). 2023 Dec 1;102(48):e36237. doi: 10.1097/MD.0000000000036237. Medicine (Baltimore). 2023. PMID: 38050254 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
