Estrogen Deprivation and Myocardial Infarction: Role of Aerobic Exercise Training, Inflammation and Metabolomics
- PMID: 31362678
- PMCID: PMC7903506
- DOI: 10.2174/1573403X15666190729153026
Estrogen Deprivation and Myocardial Infarction: Role of Aerobic Exercise Training, Inflammation and Metabolomics
Abstract
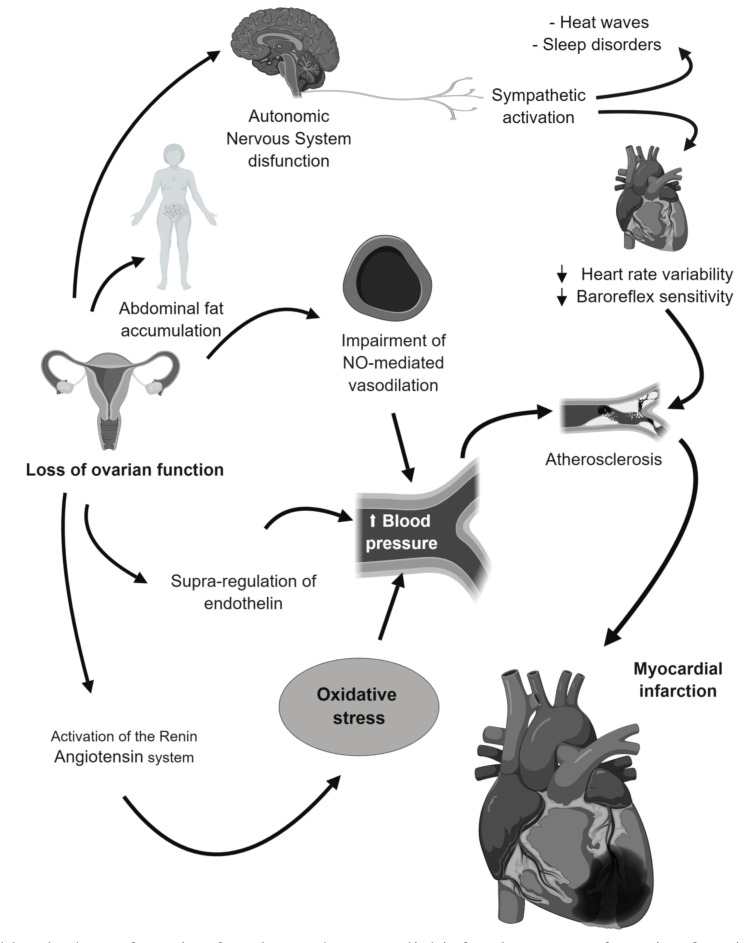
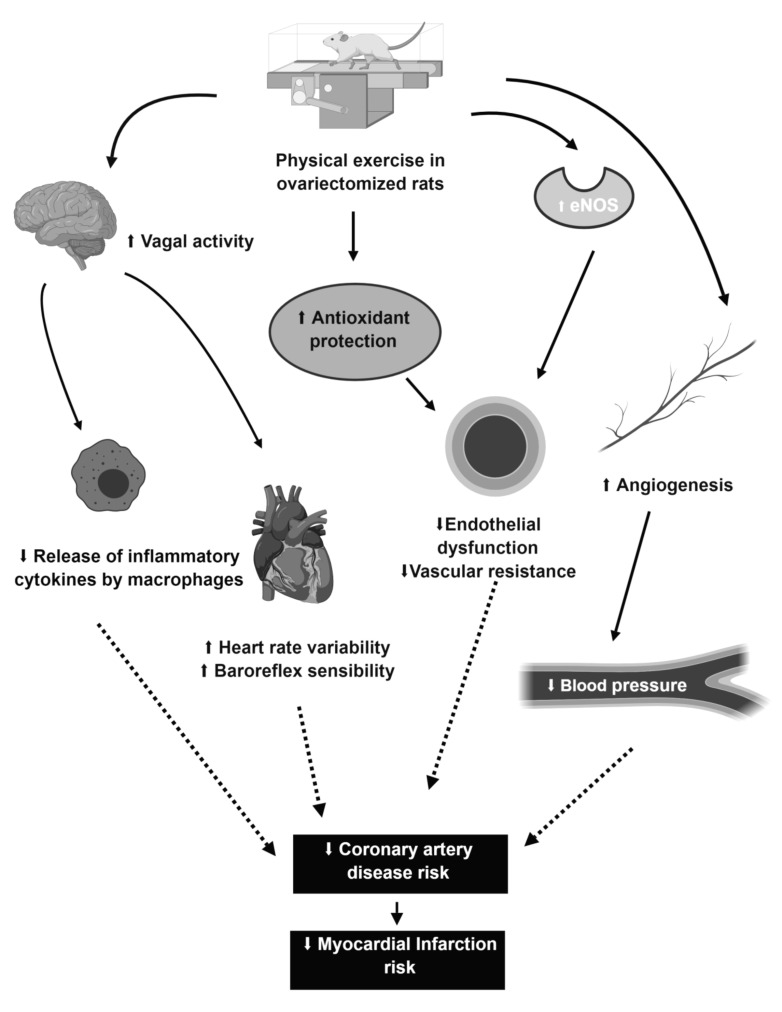
In general, postmenopausal women present higher mortality, and worse prognosis after myocardial infarction (MI) compared to men, due to estrogen deficiency. After MI, cardiovascular alterations occur such as the autonomic imbalance and the pro-inflammatory cytokines increase. In this sense, therapies that aim to minimize deleterious effects caused by myocardial ischemia are important. Aerobic training has been proposed as a promising intervention in the prevention of cardiovascular diseases. On the other hand, some studies have attempted to identify potential biomarkers for cardiovascular diseases or specifically for MI. For this purpose, metabolomics has been used as a tool in the discovery of cardiovascular biomarkers. Therefore, the objective of this work is to discuss the changes involved in ovariectomy, myocardial infarction, and aerobic training, with emphasis on inflammation and metabolism.
Keywords: Ovariectomy; aerobic training; estrogen; inflammation; metabolomics; myocardial infarction.
Copyright© Bentham Science Publishers; For any queries, please email at epub@benthamscience.net.
Figures
Similar articles
-
Aerobic training prevents cardiometabolic changes triggered by myocardial infarction in ovariectomized rats.J Cell Physiol. 2021 Feb;236(2):1105-1115. doi: 10.1002/jcp.29919. Epub 2020 Jul 7. J Cell Physiol. 2021. PMID: 32638399
-
Downregulation of miR-151-5p contributes to increased susceptibility to arrhythmogenesis during myocardial infarction with estrogen deprivation.PLoS One. 2013 Sep 9;8(9):e72985. doi: 10.1371/journal.pone.0072985. eCollection 2013. PLoS One. 2013. PMID: 24039836 Free PMC article.
-
Role of exercise training on autonomic changes and inflammatory profile induced by myocardial infarction.Mediators Inflamm. 2014;2014:702473. doi: 10.1155/2014/702473. Epub 2014 Jun 18. Mediators Inflamm. 2014. PMID: 25045212 Free PMC article. Review.
-
Exploratory metabolomic analysis for characterizing the metabolic profile of the urinary bladder under estrogen deprivation.Front Endocrinol (Lausanne). 2024 May 31;15:1384115. doi: 10.3389/fendo.2024.1384115. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38883607 Free PMC article.
-
[The role of aerobic exercise following myocardial infarction].Anadolu Kardiyol Derg. 2004 Jun;4(2):153-60. Anadolu Kardiyol Derg. 2004. PMID: 15165952 Review. Turkish.
Cited by
-
Ischemia-modified albumin: is it a promising marker in acute coronary syndrome?BMC Cardiovasc Disord. 2024 Aug 22;24(1):436. doi: 10.1186/s12872-024-04108-2. BMC Cardiovasc Disord. 2024. PMID: 39174920 Free PMC article.
-
Beyond hot flashes: Exploring the role of estrogen therapy in postmenopausal women for myocardial infarction prevention and recovery.Biomol Biomed. 2024 Jan 3;24(1):4-13. doi: 10.17305/bb.2023.9535. Biomol Biomed. 2024. PMID: 37650466 Free PMC article. Review.
-
Macrophages promote the transition from myocardial ischemia reperfusion injury to cardiac fibrosis in mice through GMCSF/CCL2/CCR2 and phenotype switching.Acta Pharmacol Sin. 2024 May;45(5):959-974. doi: 10.1038/s41401-023-01222-3. Epub 2024 Jan 15. Acta Pharmacol Sin. 2024. PMID: 38225394
-
Paraganglioma-induced reverse takotsubo syndrome treated with extracorporeal membrane oxygenation in a young patient with a history of malignancy: a case report.Eur Heart J Case Rep. 2023 Nov 24;7(12):ytad591. doi: 10.1093/ehjcr/ytad591. eCollection 2023 Dec. Eur Heart J Case Rep. 2023. PMID: 38130863 Free PMC article.
-
Erxian decoction ameliorates myocardial tissue damage through activating PI3K/AKT signaling pathway in ovariectomized rats.Ann Med. 2024 Dec;56(1):2411013. doi: 10.1080/07853890.2024.2411013. Epub 2024 Oct 9. Ann Med. 2024. PMID: 39382555 Free PMC article.
References
-
- Hage F.G., Oparil S. Ovarian hormones and vascular disease. Curr. Opin. Cardiol. 2013;28(4):411–416. - PubMed
-
- Casanova G., Pritzer P.M. Aspectos Fisiopatológicos: Estrogênios, menopausa e terapia hormonal. Revista da Sociedade Brasileira de Hipertensão. 2007;10:131–134.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical