

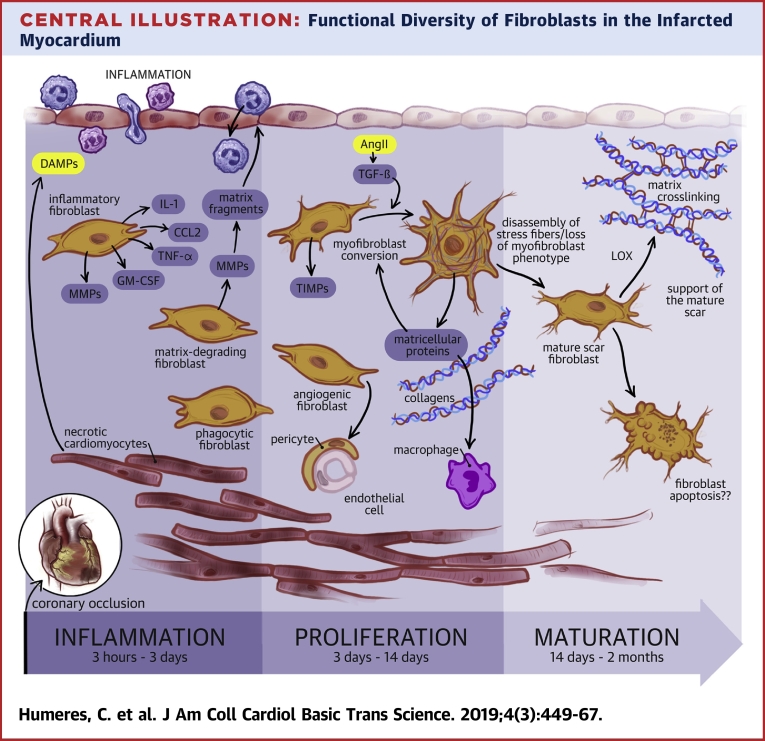
Fibroblasts in the Infarcted, Remodeling, and Failing Heart
- PMID: 31312768
- PMCID: PMC6610002
- DOI: 10.1016/j.jacbts.2019.02.006
Fibroblasts in the Infarcted, Remodeling, and Failing Heart
Abstract
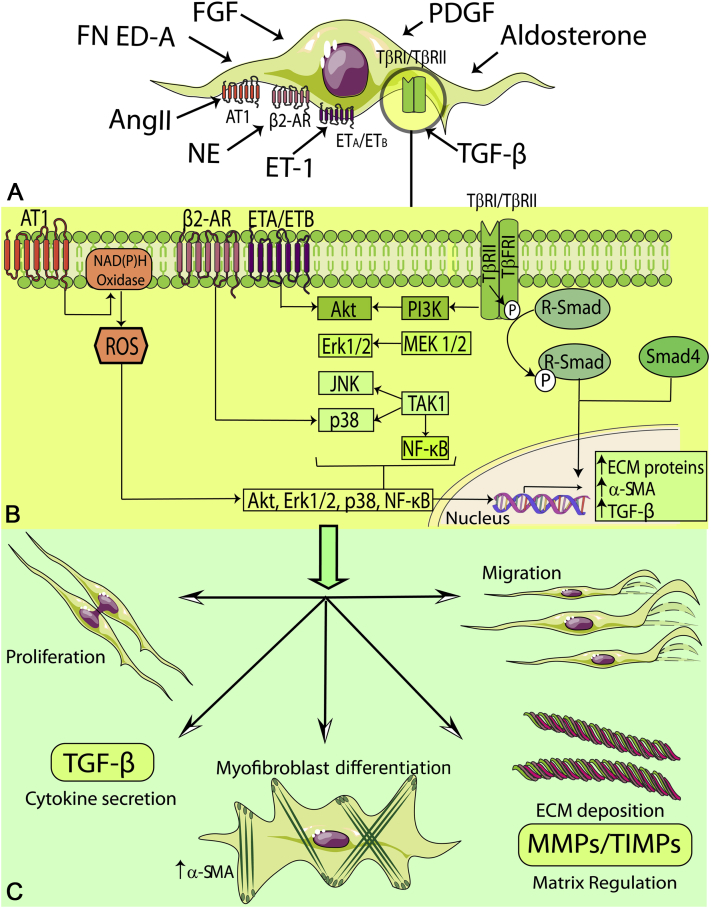
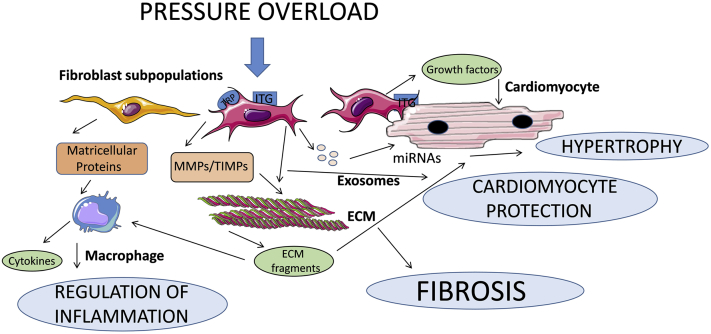
Expansion and activation of fibroblasts following cardiac injury is important for repair but may also contribute to fibrosis, remodeling, and dysfunction. The authors discuss the dynamic alterations of fibroblasts in failing and remodeling myocardium. Emerging concepts suggest that fibroblasts are not unidimensional cells that act exclusively by secreting extracellular matrix proteins, thus promoting fibrosis and diastolic dysfunction. In addition to their involvement in extracellular matrix expansion, activated fibroblasts may also exert protective actions, preserving the cardiac extracellular matrix, transducing survival signals to cardiomyocytes, and regulating inflammation and angiogenesis. The functional diversity of cardiac fibroblasts may reflect their phenotypic heterogeneity.
Keywords: AT1, angiotensin type 1; ECM, extracellular matrix; FAK, focal adhesion kinase; FGF, fibroblast growth factor; IL, interleukin; MAPK, mitogen-activated protein kinase; MRTF, myocardin-related transcription factor; PDGF, platelet-derived growth factor; RNA, ribonucleic acid; ROCK, Rho-associated coiled-coil containing kinase; ROS, reactive oxygen species; SMA, smooth muscle actin; TGF, transforming growth factor; TRP, transient receptor potential; cytokines; extracellular matrix; fibroblast; infarction; lncRNA, long noncoding ribonucleic acid; miRNA, micro–ribonucleic acid; remodeling.
Figures


Similar articles
-
Blockade of Fibroblast YAP Attenuates Cardiac Fibrosis and Dysfunction Through MRTF-A Inhibition.JACC Basic Transl Sci. 2020 Sep 28;5(9):931-945. doi: 10.1016/j.jacbts.2020.07.009. eCollection 2020 Sep. JACC Basic Transl Sci. 2020. PMID: 33015415 Free PMC article.
-
A-kinase anchoring protein-Lbc promotes pro-fibrotic signaling in cardiac fibroblasts.Biochim Biophys Acta. 2014 Feb;1843(2):335-45. doi: 10.1016/j.bbamcr.2013.11.008. Epub 2013 Nov 22. Biochim Biophys Acta. 2014. PMID: 24269843
-
Protective Effects of Activated Myofibroblasts in the Pressure-Overloaded Myocardium Are Mediated Through Smad-Dependent Activation of a Matrix-Preserving Program.Circ Res. 2019 Apr 12;124(8):1214-1227. doi: 10.1161/CIRCRESAHA.118.314438. Circ Res. 2019. PMID: 30686120 Free PMC article.
-
Cardiac fibrosis: Cell biological mechanisms, molecular pathways and therapeutic opportunities.Mol Aspects Med. 2019 Feb;65:70-99. doi: 10.1016/j.mam.2018.07.001. Epub 2018 Aug 2. Mol Aspects Med. 2019. PMID: 30056242 Review.
-
The Extracellular Matrix in Ischemic and Nonischemic Heart Failure.Circ Res. 2019 Jun 21;125(1):117-146. doi: 10.1161/CIRCRESAHA.119.311148. Epub 2019 Jun 20. Circ Res. 2019. PMID: 31219741 Free PMC article. Review.
Cited by
-
Calycosin as a Novel PI3K Activator Reduces Inflammation and Fibrosis in Heart Failure Through AKT-IKK/STAT3 Axis.Front Pharmacol. 2022 Feb 21;13:828061. doi: 10.3389/fphar.2022.828061. eCollection 2022. Front Pharmacol. 2022. PMID: 35264961 Free PMC article.
-
Cardiac Fibroblast Activation in Patients Early After Acute Myocardial Infarction: Integration with MR Tissue Characterization and Subsequent Functional Outcome.J Nucl Med. 2022 Sep;63(9):1415-1423. doi: 10.2967/jnumed.121.263555. Epub 2022 Feb 24. J Nucl Med. 2022. PMID: 35210301 Free PMC article.
-
Stamp2 Protects From Maladaptive Structural Remodeling and Systolic Dysfunction in Post-Ischemic Hearts by Attenuating Neutrophil Activation.Front Immunol. 2021 Oct 6;12:701721. doi: 10.3389/fimmu.2021.701721. eCollection 2021. Front Immunol. 2021. PMID: 34691017 Free PMC article.
-
Helium Conditioning Increases Cardiac Fibroblast Migration Which Effect Is Not Propagated via Soluble Factors or Extracellular Vesicles.Int J Mol Sci. 2021 Sep 29;22(19):10504. doi: 10.3390/ijms221910504. Int J Mol Sci. 2021. PMID: 34638845 Free PMC article.
-
WNT/β-Catenin Signaling Promotes TGF-β-Mediated Activation of Human Cardiac Fibroblasts by Enhancing IL-11 Production.Int J Mol Sci. 2021 Sep 17;22(18):10072. doi: 10.3390/ijms221810072. Int J Mol Sci. 2021. PMID: 34576234 Free PMC article.
References
-
- Frangogiannis N.G. Cardiac fibrosis: cell biological mechanisms, molecular pathways and therapeutic opportunities. Mol Aspects Med. 2019;65:70–99. - PubMed
-
- Aoki T., Fukumoto Y., Sugimura K. Prognostic impact of myocardial interstitial fibrosis in non-ischemic heart failure. Comparison between preserved and reduced ejection fraction heart failure. Circ J. 2011;75:2605–2613. - PubMed
-
- Paulus W.J., Tschope C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62:263–271. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
