

Performance of mid-upper arm circumference to diagnose acute malnutrition in a cross-sectional community-based sample of children aged 6-24 months in Niger
- PMID: 31214293
- PMCID: PMC6548705
- DOI: 10.4162/nrp.2019.13.3.247
Performance of mid-upper arm circumference to diagnose acute malnutrition in a cross-sectional community-based sample of children aged 6-24 months in Niger
Abstract
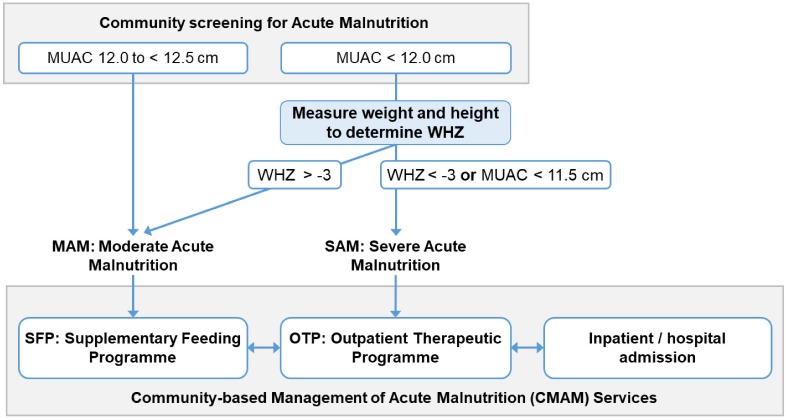
Background/objectives: Accurate, early identification of acutely malnourished children has the potential to reduce related child morbidity and mortality. The current World Health Organisation (WHO) guidelines classify non-oedematous acute malnutrition among children under five using Mid-Upper Arm Circumference (MUAC) or Weight-for-Height Z-score (WHZ). However, there is ongoing debate regarding the use of current MUAC cut-offs. This study investigates the diagnostic performance of MUAC to identify children aged 6-24 months with global (GAM) or severe acute malnutrition (SAM).
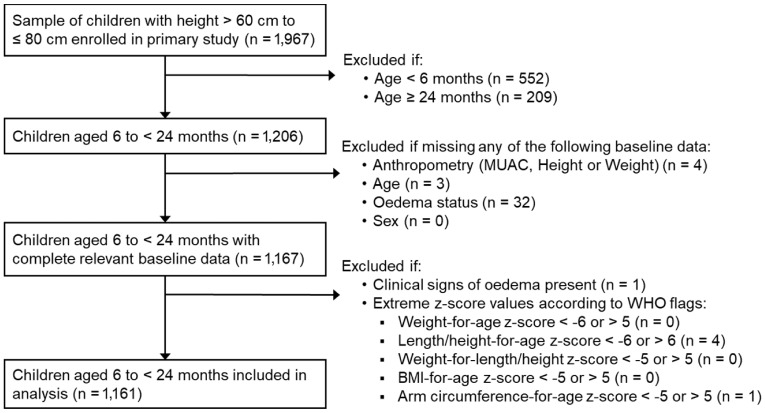
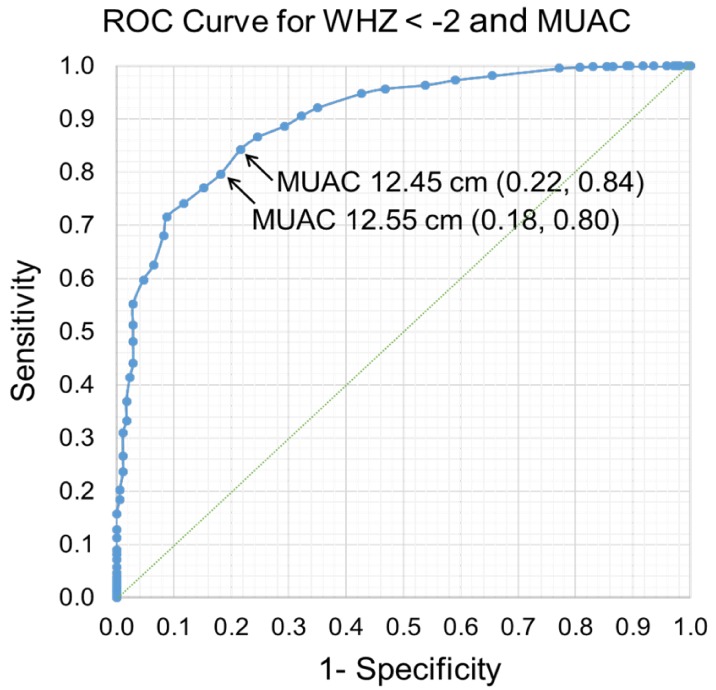
Subjects/methods: Cross-sectional, secondary data from a community sample of children aged 6-24 months in Niger were used for this study. Children with complete weight, height and MUAC data and without clinical oedema were included. Using WHO guidelines for GAM (WHZ < -2, MUAC < 12.5 cm) and SAM (WHZ < -3, MUAC < 11.5 cm), the sensitivity (Se), specificity (Sp), predictive values, Youden Index and Receiver Operating Characteristic (ROC) curves were calculated for MUAC when compared with the WHZ reference criterion.
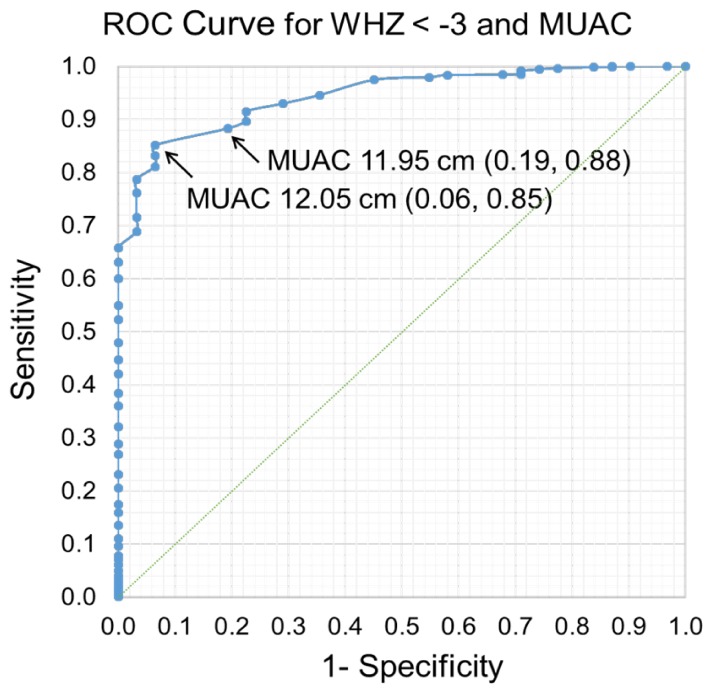
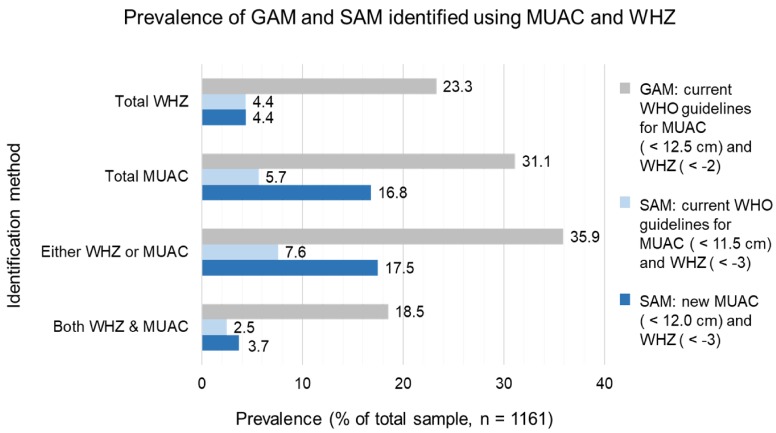
Results: Of 1161 children, 23.3% were diagnosed with GAM using WHZ, and 4.4% with SAM. Using current WHO cut-offs, the Se of MUAC to identify GAM was greater than for SAM (79 vs. 57%), yet the Sp was lower (84 vs. 97%). From inspection of the ROC curve and Youden Index, Se and Sp were maximised for MUAC < 12.5 cm to identify GAM (Se 79%, Sp 84%), and MUAC < 12.0 cm to identify SAM (Se 88%, Sp 81%).
Conclusions: The current MUAC cut-off to identify GAM should continue to be used, but when screening for SAM, a higher cut-off could improve case identification. Community screening for SAM could use MUAC < 12.0 cm followed by appropriate treatment based on either MUAC < 11.5 cm or WHZ < -3, as in current practice. While the practicalities of implementation must be considered, the higher SAM MUAC cut-off would maximise early case-finding of high-risk acutely malnourished children.
Keywords: Niger; Severe acute malnutrition; anthropometric measures; community screening; diagnosis.
Conflict of interest statement
CONFLICT OF INTEREST: SKM, JME and AE declare that they have no potential conflicts of interests. AE is employed by, and JME is affiliated to Karolinska Institutet. None of the authors received funding or specific salary for this study or publication.
Figures
Similar articles
-
Diagnostic Accuracy of Mid-Upper Arm Circumference for the Detection of Acute Malnutrition Among Children Aged 6-60 Months: A Diagnostic Accuracy Study.J Res Health Sci. 2024 Jun 1;24(2):e00612. doi: 10.34172/jrhs.2024.147. Epub 2024 Jun 1. J Res Health Sci. 2024. PMID: 39072548 Free PMC article.
-
Routinely MUAC screening for severe acute malnutrition should consider the gender and age group bias in the Ethiopian non-emergency context.PLoS One. 2020 Apr 9;15(4):e0230502. doi: 10.1371/journal.pone.0230502. eCollection 2020. PLoS One. 2020. PMID: 32271790 Free PMC article.
-
Severely malnourished children with a low weight-for-height have a higher mortality than those with a low mid-upper-arm-circumference: I. Empirical data demonstrates Simpson's paradox.Nutr J. 2018 Sep 15;17(1):79. doi: 10.1186/s12937-018-0384-4. Nutr J. 2018. PMID: 30217205 Free PMC article.
-
Sensitivity and specificity of mid-upper arm circumference for assessment of severe acute malnutrition among children ages 6 to 59 months: Systematic review and meta-analysis.Nutrition. 2023 Mar;107:111918. doi: 10.1016/j.nut.2022.111918. Epub 2022 Nov 30. Nutrition. 2023. PMID: 36566609 Review.
-
Implications of updated protocol for classification of childhood malnutrition and service delivery in world's largest refugee camp amid this COVID-19 pandemic.Public Health Nutr. 2022 Mar;25(3):538-542. doi: 10.1017/S1368980022000052. Epub 2022 Jan 12. Public Health Nutr. 2022. PMID: 35016741 Free PMC article. Review.
Cited by
-
Diagnostic Accuracy of Mid-Upper Arm Circumference for the Detection of Acute Malnutrition Among Children Aged 6-60 Months: A Diagnostic Accuracy Study.J Res Health Sci. 2024 Jun 1;24(2):e00612. doi: 10.34172/jrhs.2024.147. Epub 2024 Jun 1. J Res Health Sci. 2024. PMID: 39072548 Free PMC article.
-
Impact of Integration of Severe Acute Malnutrition Treatment in Primary Health Care Provided by Community Health Workers in Rural Niger.Nutrients. 2021 Nov 14;13(11):4067. doi: 10.3390/nu13114067. Nutrients. 2021. PMID: 34836322 Free PMC article. Clinical Trial.
-
Validity of "Mid-Upper Arm Circumference" as a Parameter to Identify Undernourished Children in Rural Gujarat.Indian J Community Med. 2024 May-Jun;49(3):475-479. doi: 10.4103/ijcm.ijcm_789_22. Epub 2024 May 24. Indian J Community Med. 2024. PMID: 38933793 Free PMC article.
-
Routinely MUAC screening for severe acute malnutrition should consider the gender and age group bias in the Ethiopian non-emergency context.PLoS One. 2020 Apr 9;15(4):e0230502. doi: 10.1371/journal.pone.0230502. eCollection 2020. PLoS One. 2020. PMID: 32271790 Free PMC article.
-
Association of Postpartum Depression with Maternal Serum Magnesium Levels, Infant Growth, and Neurodevelopmental Indices.Int J Prev Med. 2024 Mar 28;15:16. doi: 10.4103/ijpvm.ijpvm_30_24. eCollection 2024. Int J Prev Med. 2024. PMID: 38715695 Free PMC article.
References
-
- United Nations Children's Fund; World Health Organization; World Bank Group. Levels and Trends in Child Malnutrition, UNICEF - WHO - World Bank Group Joint Child Malnutrition Estimates. Geneva: World Health Organization; 2015.
-
- Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R, Uauy R Maternal and Child Nutrition Study Group. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382:427–451. - PubMed
-
- World Health Organization; United Nations Children's Fund. WHO Child Growth Standards and the Identification of Severe Acute Malnutrition in Infants and Children: a Joint Statement. Geneva: World Health Organization; 2009. - PubMed
-
- World Health Organization. Guideline: Updates on the Management of Severe Acute Malnutrition in Infants and Children. Geneva: World Health Organization; 2013. - PubMed
-
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development. Geneva: World Health Organization; 2006.
