

Predicting (side) effects for patients with inflammatory bowel disease: The promise of pharmacogenetics
- PMID: 31210708
- PMCID: PMC6558438
- DOI: 10.3748/wjg.v25.i21.2539
Predicting (side) effects for patients with inflammatory bowel disease: The promise of pharmacogenetics
Abstract
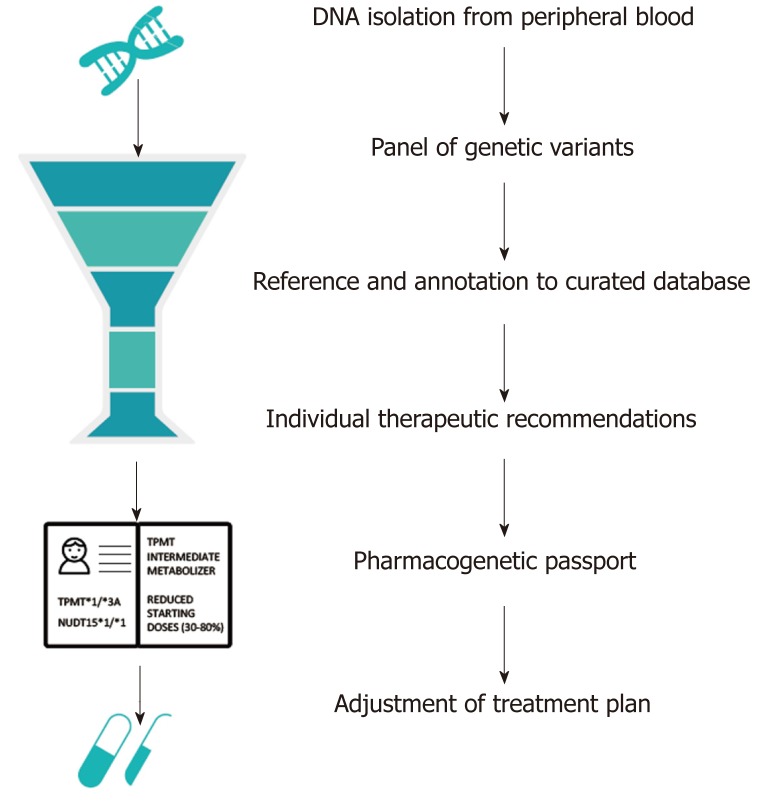
Inflammatory bowel disease (IBD) is a chronic and heterogeneous intestinal inflammatory disorder. The medical management of IBD aims for long-lasting disease remission to prevent complications and disease progression. Early introduction of immunosuppression forms the mainstay of medical IBD management. Large inter-individual variability in drug responses, in terms of both efficacy and toxicity, leads to high rates of therapeutic failure in the management of IBD. Better patient stratification is needed to maximize patient benefit and minimize the harm caused by adverse events. Pre-treatment pharmacogenetic testing has the potential to optimize drug selection and dose, and to minimize harm caused by adverse drug reactions. In addition, optimizing the use of cheap conventional drugs, and avoiding expensive ineffective drugs, will lead to a significant reduction in costs. Genetic variation in both TPMT and NUDT15, genes involved in thiopurine metabolism, is associated to an increased risk of thiopurine-induced myelosuppression. Moreover, specific HLA haplotypes confer risk to thiopurine-induced pancreatitis and to immunogenicity to tumor necrosis factor-antagonists, respectively. Falling costs and increased availability of genetic tests allow for the incorporation of pre-treatment genetic tests into clinical IBD management guidelines. In this paper, we review clinically useful pharmacogenetic associations for individualized treatment of patients with IBD and discuss the path from identification of a predictive pharmacogenetic marker to implementation into IBD clinical care.
Keywords: Crohn’s disease; Inflammatory bowel disease; Personalized medicine; Pharmacogenetics; Ulcerative colitis.
Conflict of interest statement
Conflict-of-interest statement: R.K.W. received unrestricted research grants from Takeda, Tramedico and Ferring. E.A.M.F. received an unrestricted research grant from Takeda. The remaining authors disclose no conflicts.
Figures
Similar articles
-
Predicted efficacy of a pharmacogenetic passport for inflammatory bowel disease.Aliment Pharmacol Ther. 2020 Jun;51(11):1105-1115. doi: 10.1111/apt.15762. Epub 2020 May 3. Aliment Pharmacol Ther. 2020. PMID: 32363635 Free PMC article.
-
Update on thiopurine pharmacogenetics in inflammatory bowel disease.Pharmacogenomics. 2015 Jul;16(8):891-903. doi: 10.2217/pgs.15.29. Epub 2015 Jun 12. Pharmacogenomics. 2015. PMID: 26067482 Review.
-
Review article: the benefits of pharmacogenetics for improving thiopurine therapy in inflammatory bowel disease.Aliment Pharmacol Ther. 2012 Jan;35(1):15-36. doi: 10.1111/j.1365-2036.2011.04905.x. Epub 2011 Nov 2. Aliment Pharmacol Ther. 2012. PMID: 22050052 Review.
-
A pharmacogenetics study of TPMT and ITPA genes detects a relationship with side effects and clinical response in patients with inflammatory bowel disease receiving Azathioprine.J Gastrointestin Liver Dis. 2011 Sep;20(3):247-53. J Gastrointestin Liver Dis. 2011. PMID: 21961091
-
Time to incorporate preemptive NUDT15 testing before starting thiopurines in inflammatory bowel disease in Asia and beyond: a review.Expert Rev Clin Pharmacol. 2023 Jul-Dec;16(7):643-653. doi: 10.1080/17512433.2023.2232300. Epub 2023 Jul 5. Expert Rev Clin Pharmacol. 2023. PMID: 37387532 Review.
Cited by
-
Cytotoxicity of Thiopurine Drugs in Patients with Inflammatory Bowel Disease.Toxics. 2022 Mar 22;10(4):151. doi: 10.3390/toxics10040151. Toxics. 2022. PMID: 35448412 Free PMC article. Review.
-
Polygenetic risk scores do not add predictive power to clinical models for response to anti-TNFα therapy in inflammatory bowel disease.PLoS One. 2021 Sep 17;16(9):e0256860. doi: 10.1371/journal.pone.0256860. eCollection 2021. PLoS One. 2021. PMID: 34534227 Free PMC article.
-
Quantification of deoxythioguanosine in human DNA with LC-MS/MS, a marker for thiopurine therapy optimisation.Anal Bioanal Chem. 2024 Dec;416(29):6711-6723. doi: 10.1007/s00216-024-05581-6. Epub 2024 Oct 13. Anal Bioanal Chem. 2024. PMID: 39397163 Free PMC article.
-
Identification of the informational and supportive needs of patients diagnosed with inflammatory bowel disease: a scoping review.Front Psychol. 2023 May 11;14:1055449. doi: 10.3389/fpsyg.2023.1055449. eCollection 2023. Front Psychol. 2023. PMID: 37251032 Free PMC article.
-
Pretreatment HLADQA1-HLADRB1 Testing for the Prevention of Azathioprine-Induced Pancreatitis in Inflammatory Bowel Disease: A Prospective Cohort Study.Clin Transl Gastroenterol. 2021 Apr 5;12(4):e00332. doi: 10.14309/ctg.0000000000000332. Clin Transl Gastroenterol. 2021. PMID: 33821842 Free PMC article.
References
-
- Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142:46–54.e42; quiz e30. - PubMed
-
- Louis E, Vermeire S, Rutgeerts P, De Vos M, Van Gossum A, Pescatore P, Fiasse R, Pelckmans P, Reynaert H, D'Haens G, Malaise M, Belaiche J. A positive response to infliximab in Crohn disease: Association with a higher systemic inflammation before treatment but not with -308 TNF gene polymorphism. Scand J Gastroenterol. 2002;37:818–824. - PubMed
-
- Vermeire S, Louis E, Carbonez A, Van Assche G, Noman M, Belaiche J, De Vos M, Van Gossum A, Pescatore P, Fiasse R, Pelckmans P, Reynaert H, D'Haens G, Rutgeerts P Belgian Group of Infliximab Expanded Access Program in Crohn's Disease. Demographic and clinical parameters influencing the short-term outcome of anti-tumor necrosis factor (infliximab) treatment in Crohn's disease. Am J Gastroenterol. 2002;97:2357–2363. - PubMed
-
- Parsi MA, Achkar JP, Richardson S, Katz J, Hammel JP, Lashner BA, Brzezinski A. Predictors of response to infliximab in patients with Crohn's disease. Gastroenterology. 2002;123:707–713. - PubMed
-
- Arnott ID, McNeill G, Satsangi J. An analysis of factors influencing short-term and sustained response to infliximab treatment for Crohn's disease. Aliment Pharmacol Ther. 2003;17:1451–1457. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
