

Reliability and safety of minimally invasive esophagectomy after neoadjuvant chemoradiation: a retrospective study
- PMID: 31138245
- PMCID: PMC6537410
- DOI: 10.1186/s13019-019-0920-0
Reliability and safety of minimally invasive esophagectomy after neoadjuvant chemoradiation: a retrospective study
Abstract
Background: Thoracic surgeons have recognized the advantages of minimally invasive esophagectomy (MIE). However, MIE for locally advanced esophageal cancer after neoadjuvant chemoradiotherapy (NCRT) is controversial. This study aimed to nvestigate and summarise the reliability and safety of MIE after NCRT.
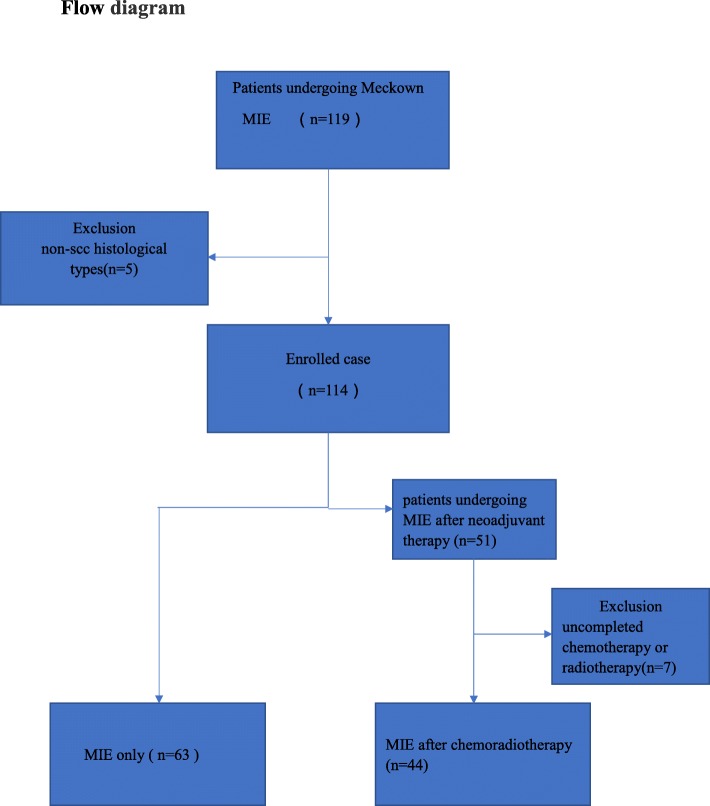
Methods: We retrospectively analyzed the perioperative outcomes of patients with locally advanced esophageal cancer who underwent minimally invasive esophagectomy after neoadjuvant chemoradiotherapy from January 2016 to January 2018, and compared them with patients who underwent MIE alone during the same period.
Results: In total, 107 patients were eligible for the study. Forty-four patients underwent MIE after NCRT (CRM), and 63 patients underwent MIE alone (MA). The surgical duration (253.59 ± 47.51 vs. 222.86 ± 42.86 min), intraoperative blood loss (164.55 ± 109.09 vs. 146.19 ± 112.89 ml), number of lymph nodes resected (18.36 ± 8.01 vs. 22.10 ± 12.03), duration of the postoperative hospital stay (12.84 ± 6.57 vs. 14.60 ± 8.48 days), postoperative intubation time (5.68 ± 3.08 vs. 6.54 ± 4.97 days), total incidence of complications (34.10% vs. 31.7%), and R0 resection rate (95.45% vs. 96.83%) had no significant difference. The incidence of arrhythmia was higher in CRM (P < 0.02). No mortality occurred postoperatively within 30 days in either group.
Conclusion: Minimally invasive esophagectomy after neoadjuvant chemoradiotherapy is a feasible, safe, and beneficial for postoperative recovery of patients.
Keywords: Esophageal squamous cell carcinoma (ESCC); Locally advanced esophageal cancer; Minimally invasive esophagectomy (MIE); Neoadjuvant chemoradiotherapy (NCRT).
Conflict of interest statement
The authors declare that they have no competing interests.
Similar articles
-
Morbidity and Mortality of Patients Who Underwent Minimally Invasive Esophagectomy After Neoadjuvant Chemoradiotherapy vs Neoadjuvant Chemotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Randomized Clinical Trial.JAMA Surg. 2021 May 1;156(5):444-451. doi: 10.1001/jamasurg.2021.0133. JAMA Surg. 2021. PMID: 33729467 Free PMC article. Clinical Trial.
-
CMISG1701: a multicenter prospective randomized phase III clinical trial comparing neoadjuvant chemoradiotherapy to neoadjuvant chemotherapy followed by minimally invasive esophagectomy in patients with locally advanced resectable esophageal squamous cell carcinoma (cT3-4aN0-1M0) (NCT03001596).BMC Cancer. 2017 Jun 28;17(1):450. doi: 10.1186/s12885-017-3446-7. BMC Cancer. 2017. PMID: 28659128 Free PMC article. Clinical Trial.
-
Outcomes With Open and Minimally Invasive Ivor Lewis Esophagectomy After Neoadjuvant Therapy.Ann Thorac Surg. 2016 Mar;101(3):1097-103. doi: 10.1016/j.athoracsur.2015.09.062. Epub 2015 Dec 1. Ann Thorac Surg. 2016. PMID: 26652140
-
Robotic Versus Conventional Minimally Invasive Esophagectomy for Esophageal Cancer: A Meta-analysis.Ann Surg. 2023 Jul 1;278(1):39-50. doi: 10.1097/SLA.0000000000005782. Epub 2022 Dec 20. Ann Surg. 2023. PMID: 36538615 Review.
-
Impact of Neoadjuvant Chemoradiation on Short-Term Outcomes for Esophageal Squamous Cell Carcinoma Patients: A Meta-analysis.Ann Surg Oncol. 2016 Oct;23(11):3632-3640. doi: 10.1245/s10434-016-5298-9. Epub 2016 Jun 8. Ann Surg Oncol. 2016. PMID: 27278203 Review.
Cited by
-
Minimally invasive oesophagectomy with a total two-field lymphadenectomy after neoadjuvant chemoradiotherapy for locally advanced squamous cell carcinoma of the oesophagus: A prospective study.J Minim Access Surg. 2021 Jan-Mar;17(1):49-55. doi: 10.4103/jmas.JMAS_242_19. J Minim Access Surg. 2021. PMID: 31929228 Free PMC article.
-
Feasibility, safety and oncological outcomes of minimally invasive oesophagectomy following neoadjuvant chemoradiotherapy for oesophageal squamous cell carcinoma - Experience from a tertiary care centre.J Minim Access Surg. 2022 Oct-Dec;18(4):545-556. doi: 10.4103/jmas.jmas_242_21. J Minim Access Surg. 2022. PMID: 36124466 Free PMC article.
-
Comparison of neoadjuvant chemotherapy or chemoradiotherapy plus immunotherapy for locally resectable esophageal squamous cell carcinoma.Front Immunol. 2024 May 8;15:1336798. doi: 10.3389/fimmu.2024.1336798. eCollection 2024. Front Immunol. 2024. PMID: 38779667 Free PMC article.
-
Robot-Assisted Esophagectomy After Neoadjuvant Chemoradiation-Current Status and Future Prospects.Indian J Surg Oncol. 2020 Dec;11(4):668-673. doi: 10.1007/s13193-020-01230-3. Epub 2020 Sep 25. Indian J Surg Oncol. 2020. PMID: 33281406 Free PMC article. Review.
-
Feasibility research of enhanced recovery after surgery implemented in esophageal cancer patients who underwent neoadjuvant chemotherapy.World J Surg Oncol. 2022 Jul 25;20(1):239. doi: 10.1186/s12957-022-02701-3. World J Surg Oncol. 2022. PMID: 35879767 Free PMC article.
References
-
- Van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, Richel DJ, Nieuwenhuijzen GA, Hospers GA, Bonenkamp JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366:2074–2084. doi: 10.1056/NEJMoa1112088. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
