

Brain Injury-Mediated Neuroinflammatory Response and Alzheimer's Disease
- PMID: 31092147
- PMCID: PMC7274851
- DOI: 10.1177/1073858419848293
Brain Injury-Mediated Neuroinflammatory Response and Alzheimer's Disease
Abstract
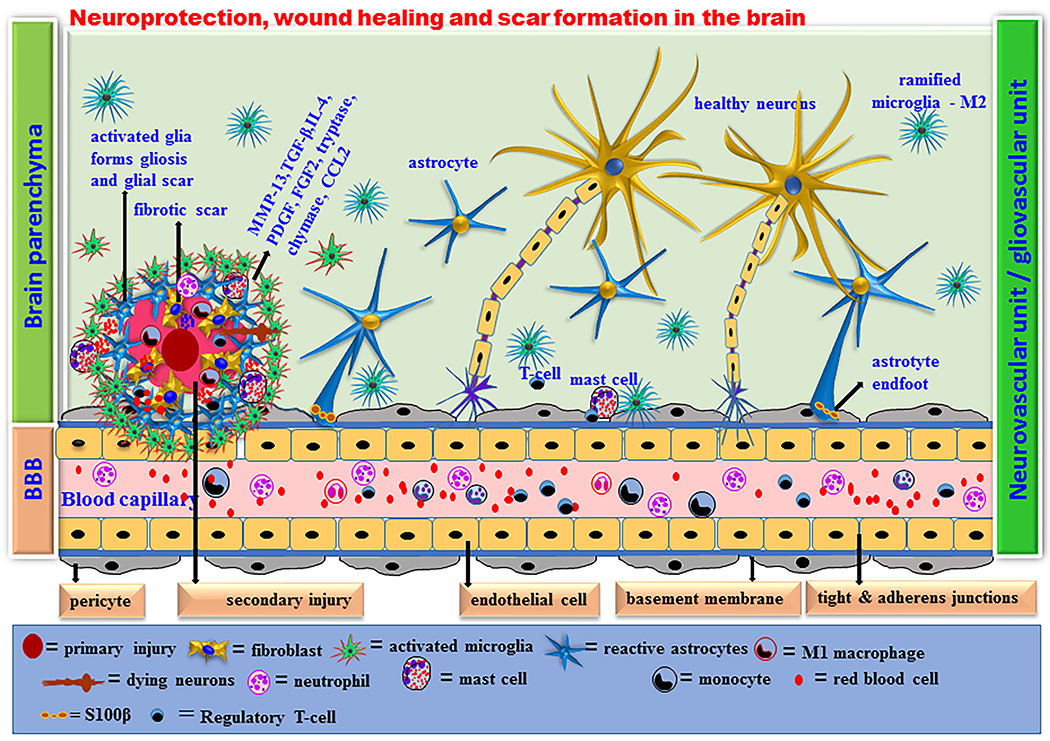
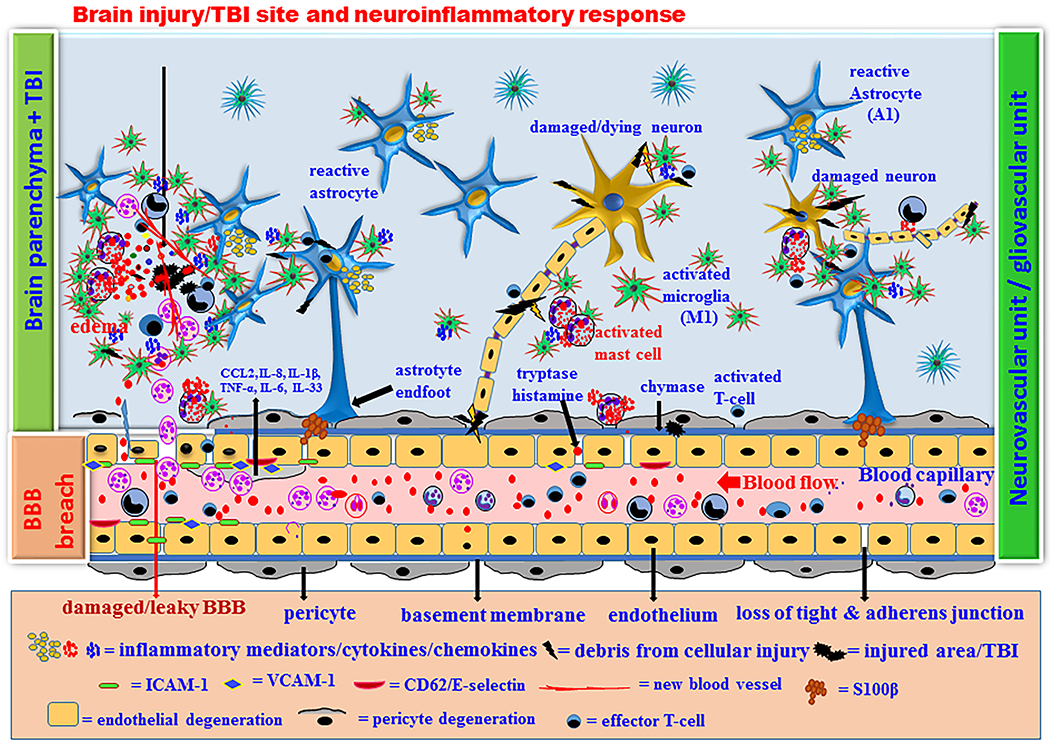
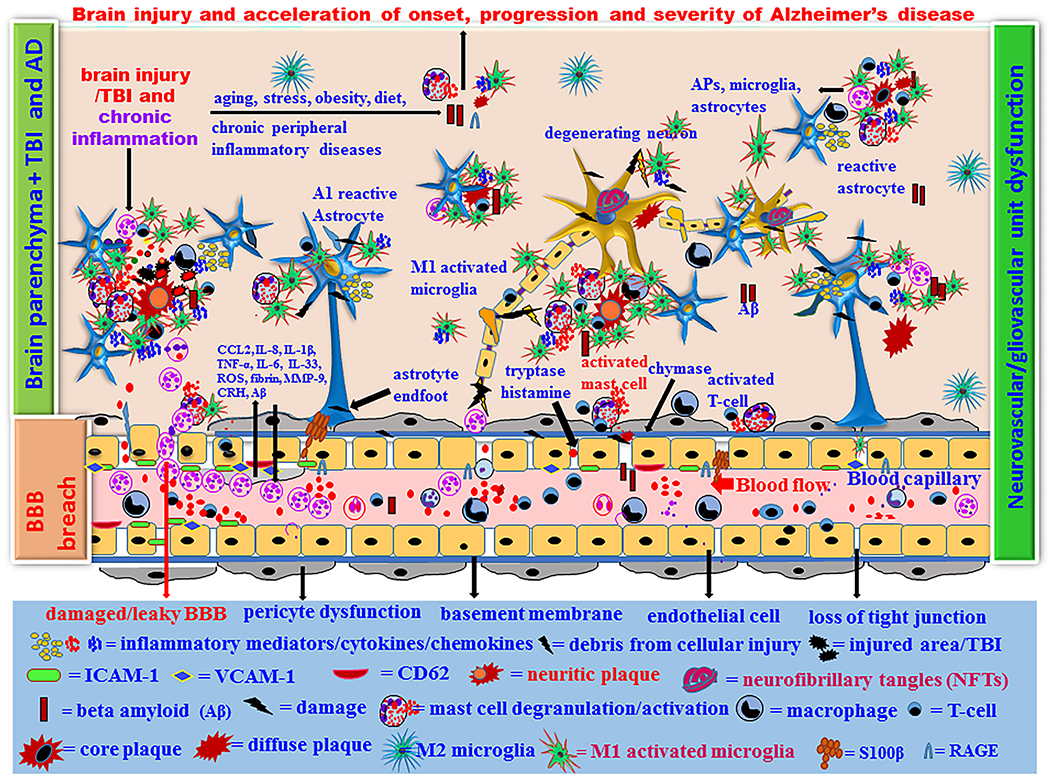
Traumatic brain injury (TBI) is a major health problem in the United States, which affects about 1.7 million people each year. Glial cells, T-cells, and mast cells perform specific protective functions in different regions of the brain for the recovery of cognitive and motor functions after central nervous system (CNS) injuries including TBI. Chronic neuroinflammatory responses resulting in neuronal death and the accompanying stress following brain injury predisposes or accelerates the onset and progression of Alzheimer's disease (AD) in high-risk individuals. About 5.7 million Americans are currently living with AD. Immediately following brain injury, mast cells respond by releasing prestored and preactivated mediators and recruit immune cells to the CNS. Blood-brain barrier (BBB), tight junction and adherens junction proteins, neurovascular and gliovascular microstructural rearrangements, and dysfunction associated with increased trafficking of inflammatory mediators and inflammatory cells from the periphery across the BBB leads to increase in the chronic neuroinflammatory reactions following brain injury. In this review, we advance the hypothesis that neuroinflammatory responses resulting from mast cell activation along with the accompanying risk factors such as age, gender, food habits, emotional status, stress, allergic tendency, chronic inflammatory diseases, and certain drugs can accelerate brain injury-associated neuroinflammation, neurodegeneration, and AD pathogenesis.
Keywords: Alzheimer’s disease; blood-brain barrier; brain injury; neuroinflammation; traumatic brain injury.
Conflict of interest statement
Declaration of Conflict of Interests
The authors declare no conflict of interest.
Figures
Similar articles
-
Mast Cell Activation, Neuroinflammation, and Tight Junction Protein Derangement in Acute Traumatic Brain Injury.Mediators Inflamm. 2020 Jun 24;2020:4243953. doi: 10.1155/2020/4243953. eCollection 2020. Mediators Inflamm. 2020. PMID: 32684835 Free PMC article.
-
Altered Neuroinflammation and Behavior after Traumatic Brain Injury in a Mouse Model of Alzheimer's Disease.J Neurotrauma. 2016 Apr 1;33(7):625-40. doi: 10.1089/neu.2015.3970. Epub 2015 Nov 23. J Neurotrauma. 2016. PMID: 26414955 Free PMC article.
-
Mast Cell Activation in Brain Injury, Stress, and Post-traumatic Stress Disorder and Alzheimer's Disease Pathogenesis.Front Neurosci. 2017 Dec 12;11:703. doi: 10.3389/fnins.2017.00703. eCollection 2017. Front Neurosci. 2017. PMID: 29302258 Free PMC article. Review.
-
Brain and Peripheral Atypical Inflammatory Mediators Potentiate Neuroinflammation and Neurodegeneration.Front Cell Neurosci. 2017 Jul 24;11:216. doi: 10.3389/fncel.2017.00216. eCollection 2017. Front Cell Neurosci. 2017. PMID: 28790893 Free PMC article. Review.
-
Acute Traumatic Brain Injury-Induced Neuroinflammatory Response and Neurovascular Disorders in the Brain.Neurotox Res. 2021 Apr;39(2):359-368. doi: 10.1007/s12640-020-00288-9. Epub 2020 Sep 21. Neurotox Res. 2021. PMID: 32955722 Free PMC article.
Cited by
-
Neuroimmune connections between corticotropin-releasing hormone and mast cells: novel strategies for the treatment of neurodegenerative diseases.Neural Regen Res. 2021 Nov;16(11):2184-2197. doi: 10.4103/1673-5374.310608. Neural Regen Res. 2021. PMID: 33818491 Free PMC article. Review.
-
Potential Role of Moesin in Regulating Mast Cell Secretion.Int J Mol Sci. 2023 Jul 28;24(15):12081. doi: 10.3390/ijms241512081. Int J Mol Sci. 2023. PMID: 37569454 Free PMC article. Review.
-
Differential Retinal Protein Expression in Primary and Secondary Retinal Ganglion Cell Degeneration Identified by Integrated SWATH and Target-Based Proteomics.Int J Mol Sci. 2021 Aug 10;22(16):8592. doi: 10.3390/ijms22168592. Int J Mol Sci. 2021. PMID: 34445296 Free PMC article.
-
Perioperative neurocognitive dysfunction: thinking from the gut?Aging (Albany NY). 2020 Aug 15;12(15):15797-15817. doi: 10.18632/aging.103738. Epub 2020 Aug 15. Aging (Albany NY). 2020. PMID: 32805716 Free PMC article.
-
Metabolomics Analysis of Hippocampus and Cortex in a Rat Model of Traumatic Brain Injury in the Subacute Phase.Front Neurosci. 2020 Sep 4;14:876. doi: 10.3389/fnins.2020.00876. eCollection 2020. Front Neurosci. 2020. PMID: 33013291 Free PMC article.
References
-
- Al-Dahhak R, Khoury R, Qazi E, Grossberg GT. 2018. Traumatic Brain Injury, Chronic Traumatic Encephalopathy, and Alzheimer Disease. Clin Geriatr Med 34(4):617–635. - PubMed
-
- Amara J, Iverson KM, Krengel M, Pogoda TK, Hendricks A. 2014. Anticipating the traumatic brain injury-related health care needs of women veterans after the Department of Defense change in combat assignment policy. Womens Health Issues 24(2):e171–6. - PubMed
-
- Amoroso T, Iverson KM. 2017. Acknowledging the Risk for Traumatic Brain Injury in Women Veterans. J Nerv Ment Dis 205(4):318–323. - PubMed
-
- Anada RP, Wong KT, Jayapalan JJ, Hashim OH, Ganesan D. 2018. Panel of serum protein biomarkers to grade the severity of traumatic brain injury. Electrophoresis 39(18):2308–2315. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
