

The influence of age-associated comorbidities on responses to combination antiretroviral therapy in older people living with HIV
- PMID: 30803162
- PMCID: PMC6389354
- DOI: 10.1002/jia2.25228
The influence of age-associated comorbidities on responses to combination antiretroviral therapy in older people living with HIV
Abstract
Introduction: Multiple comorbidities among HIV-positive individuals may increase the potential for polypharmacy causing drug-to-drug interactions and older individuals with comorbidities, particularly those with cognitive impairment, may have difficulty in adhering to complex medications. However, the effects of age-associated comorbidities on the treatment outcomes of combination antiretroviral therapy (cART) are not well known. In this study, we investigated the effects of age-associated comorbidities on therapeutic outcomes of cART in HIV-positive adults in Asian countries.
Methods: Patients enrolled in the TREAT Asia HIV Observational Database cohort and on cART for more than six months were analysed. Comorbidities included hypertension, diabetes, dyslipidaemia and impaired renal function. Treatment outcomes of patients ≥50 years of age with comorbidities were compared with those <50 years and those ≥50 years without comorbidities. We analysed 5411 patients with virological failure and 5621 with immunologic failure. Our failure outcomes were defined to be in-line with the World Health Organization 2016 guidelines. Cox regression analysis was used to analyse time to first virological and immunological failure.
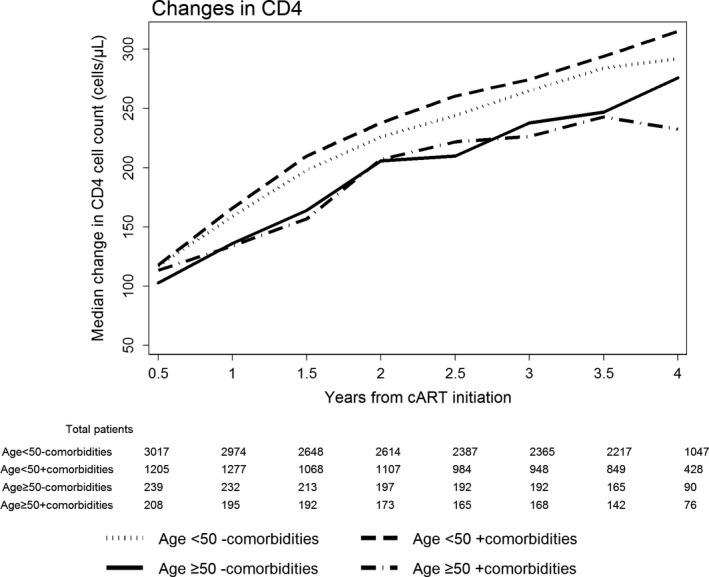
Results: The incidence of virologic failure was 7.72/100 person-years. Virological failure was less likely in patients with better adherence and higher CD4 count at cART initiation. Those acquiring HIV through intravenous drug use were more likely to have virological failure compared to those infected through heterosexual contact. On univariate analysis, patients aged <50 years without comorbidities were more likely to experience virological failure than those aged ≥50 years with comorbidities (hazard ratio 1.75, 95% confidence interval (CI) 1.31 to 2.33, p < 0.001). However, the multivariate model showed that age-related comorbidities were not significant factors for virological failure (hazard ratio 1.31, 95% CI 0.98 to 1.74, p = 0.07). There were 391 immunological failures, with an incidence of 2.75/100 person-years. On multivariate analysis, those aged <50 years without comorbidities (p = 0.025) and age <50 years with comorbidities (p = 0.001) were less likely to develop immunological failure compared to those aged ≥50 years with comorbidities.
Conclusions: In our Asia regional cohort, age-associated comorbidities did not affect virologic outcomes of cART. Among those with comorbidities, patients <50 years old showed a better CD4 response.
Keywords: HIV; cART; TAHOD (TREAT Asia HIV Observational Database); age-associated comorbidity; immunological failure; virological failure.
© 2019 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
Similar articles
-
A Decade of Combination Antiretroviral Treatment in Asia: The TREAT Asia HIV Observational Database Cohort.AIDS Res Hum Retroviruses. 2016 Aug;32(8):772-81. doi: 10.1089/AID.2015.0294. Epub 2016 May 3. AIDS Res Hum Retroviruses. 2016. PMID: 27030657 Free PMC article.
-
Deferred modification of antiretroviral regimen following documented treatment failure in Asia: results from the TREAT Asia HIV Observational Database (TAHOD).HIV Med. 2010 Jan;11(1):31-9. doi: 10.1111/j.1468-1293.2009.00738.x. Epub 2009 Jul 6. HIV Med. 2010. PMID: 19601993 Free PMC article.
-
Trends in mortality among ART-treated HIV-infected adults in the Asia-Pacific region between 1999 and 2017: results from the TREAT Asia HIV Observational Database (TAHOD) and Australian HIV Observational Database (AHOD) of IeDEA Asia-Pacific.J Int AIDS Soc. 2019 Jan;22(1):e25219. doi: 10.1002/jia2.25219. J Int AIDS Soc. 2019. PMID: 30615271 Free PMC article.
-
Optimisation of antiretroviral therapy in HIV-infected children under 3 years of age.Cochrane Database Syst Rev. 2014 May 22;2014(5):CD004772. doi: 10.1002/14651858.CD004772.pub4. Cochrane Database Syst Rev. 2014. PMID: 24852077 Free PMC article. Review.
-
Optimal time for initiating antiretroviral therapy (ART) in HIV-infected, treatment-naive children aged 2 to 5 years old.Cochrane Database Syst Rev. 2013 Oct 10;10(10):CD010309. doi: 10.1002/14651858.CD010309.pub2. Cochrane Database Syst Rev. 2013. PMID: 24114324 Free PMC article. Review.
Cited by
-
Assessment of Metabolic, Inflammatory, and Immunological Disorders Using a New Panel of Plasma Parameters in People Living with HIV Undergoing Antiretroviral Therapy-A Retrospective Study.J Clin Med. 2024 Aug 5;13(15):4580. doi: 10.3390/jcm13154580. J Clin Med. 2024. PMID: 39124846 Free PMC article.
-
The Influence of Age-Associated Comorbidities on Responses to Combination Antiretroviral Therapy Among People Living with HIV, at the ART Clinic of Jimma Medical Center, Ethiopia: A Hospital-Based Nested Case-Control Study.HIV AIDS (Auckl). 2023 Aug 9;15:457-475. doi: 10.2147/HIV.S421523. eCollection 2023. HIV AIDS (Auckl). 2023. PMID: 37583543 Free PMC article.
-
Prevalence of and prognosis for poor immunological recovery by virally suppressed and aged HIV-infected patients.Front Med (Lausanne). 2023 Oct 19;10:1259871. doi: 10.3389/fmed.2023.1259871. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37928477 Free PMC article.
-
Effects of Chinese Medicine on the Survival of AIDS Patients Administered Second-Line ART in Rural Areas of China: A Retrospective Cohort Study Based on Real-World Data.Evid Based Complement Alternat Med. 2022 Jan 27;2022:5103768. doi: 10.1155/2022/5103768. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 35126600 Free PMC article.
-
Accessing HIV care may lead to earlier ascertainment of comorbidities in health care clients in Khayelitsha, Cape Town.PLOS Glob Public Health. 2021 Dec 22;1(12):e0000031. doi: 10.1371/journal.pgph.0000031. eCollection 2021. PLOS Glob Public Health. 2021. PMID: 36962101 Free PMC article.
References
-
- Weber R, Ruppik M, Rickenbach M, Spoerri A, Furrer H, Battegay M, et al. Decreasing mortality and changing patterns of causes of death in the Swiss HIV Cohort Study. HIV Med. 2013;14(4):195–207. - PubMed
-
- Wada N, Jacobson LP, Cohen M, French A, Phair J, Munoz A. Cause‐specific life expectancies after 35 years of age for human immunodeficiency syndrome‐infected and human immunodeficiency syndrome‐negative individuals followed simultaneously in long‐term cohort studies, 1984‐2008. Am J Epidemiol. 2013;177(2):116–25. - PMC - PubMed
-
- Joint United Nations Programme on HIV/AIDS . The Gap Report. 2014. Sep [cited 2015 May 20]. Available from: http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
