

Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma
- PMID: 30779531
- PMCID: PMC6716603
- DOI: 10.1056/NEJMoa1816047
Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma
Abstract
Background: In a single-group, phase 1b trial, avelumab plus axitinib resulted in objective responses in patients with advanced renal-cell carcinoma. This phase 3 trial involving previously untreated patients with advanced renal-cell carcinoma compared avelumab plus axitinib with the standard-of-care sunitinib.
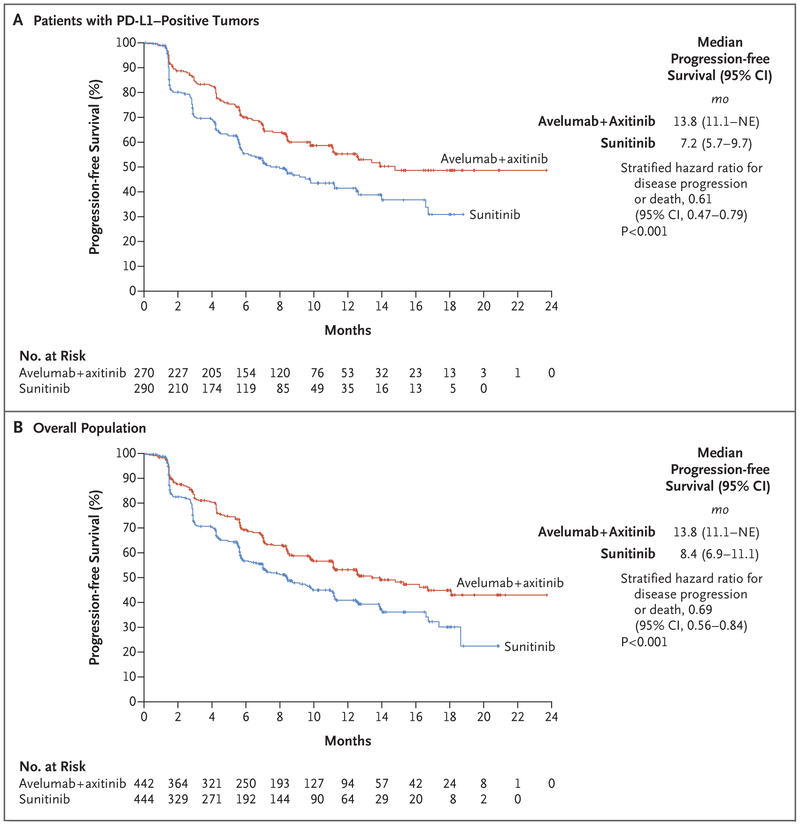
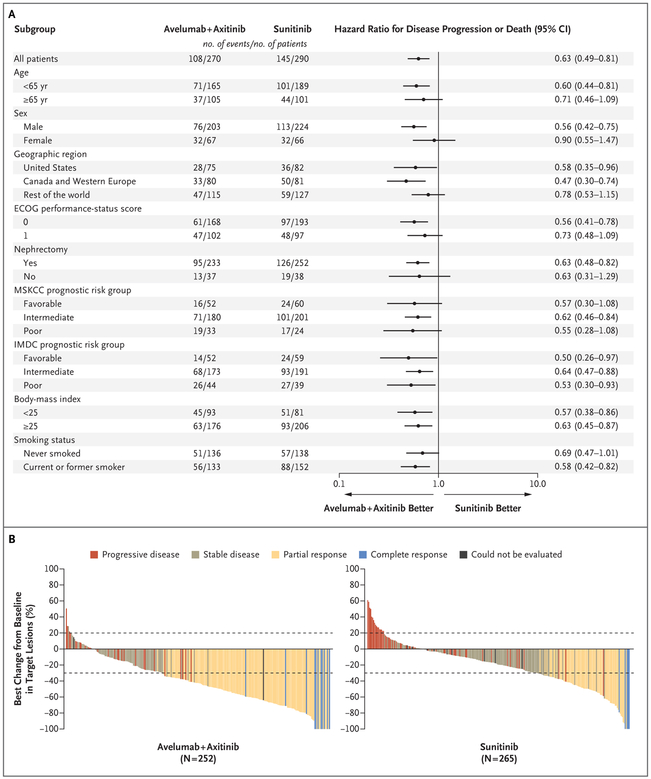
Methods: We randomly assigned patients in a 1:1 ratio to receive avelumab (10 mg per kilogram of body weight) intravenously every 2 weeks plus axitinib (5 mg) orally twice daily or sunitinib (50 mg) orally once daily for 4 weeks (6-week cycle). The two independent primary end points were progression-free survival and overall survival among patients with programmed death ligand 1 (PD-L1)-positive tumors. A key secondary end point was progression-free survival in the overall population; other end points included objective response and safety.
Results: A total of 886 patients were assigned to receive avelumab plus axitinib (442 patients) or sunitinib (444 patients). Among the 560 patients with PD-L1-positive tumors (63.2%), the median progression-free survival was 13.8 months with avelumab plus axitinib, as compared with 7.2 months with sunitinib (hazard ratio for disease progression or death, 0.61; 95% confidence interval [CI], 0.47 to 0.79; P<0.001); in the overall population, the median progression-free survival was 13.8 months, as compared with 8.4 months (hazard ratio, 0.69; 95% CI, 0.56 to 0.84; P<0.001). Among the patients with PD-L1-positive tumors, the objective response rate was 55.2% with avelumab plus axitinib and 25.5% with sunitinib; at a median follow-up for overall survival of 11.6 months and 10.7 months in the two groups, 37 patients and 44 patients had died, respectively. Adverse events during treatment occurred in 99.5% of patients in the avelumab-plus-axitinib group and in 99.3% of patients in the sunitinib group; these events were grade 3 or higher in 71.2% and 71.5% of the patients in the respective groups.
Conclusions: Progression-free survival was significantly longer with avelumab plus axitinib than with sunitinib among patients who received these agents as first-line treatment for advanced renal-cell carcinoma. (Funded by Pfizer and Merck [Darmstadt, Germany]; JAVELIN Renal 101 ClinicalTrials.gov number, NCT02684006.).
Copyright © 2019 Massachusetts Medical Society.
Figures
Comment in
-
Combination Therapy as First-Line Treatment in Metastatic Renal-Cell Carcinoma.N Engl J Med. 2019 Mar 21;380(12):1176-1178. doi: 10.1056/NEJMe1900887. Epub 2019 Feb 16. N Engl J Med. 2019. PMID: 30779526 No abstract available.
-
Immune-based combination therapy for metastatic kidney cancer.Nat Rev Nephrol. 2019 Jun;15(6):324-325. doi: 10.1038/s41581-019-0149-0. Nat Rev Nephrol. 2019. PMID: 30992548 No abstract available.
-
Immune Checkpoint Blockade plus Axitinib for Renal-Cell Carcinoma.N Engl J Med. 2019 Jun 27;380(26):2581. doi: 10.1056/NEJMc1905518. N Engl J Med. 2019. PMID: 31242369 No abstract available.
-
Immune Checkpoint Blockade plus Axitinib for Renal-Cell Carcinoma. Reply.N Engl J Med. 2019 Jun 27;380(26):2582. doi: 10.1056/NEJMc1905518. N Engl J Med. 2019. PMID: 31242371 No abstract available.
-
The tango of immunotherapy and targeted therapy in metastatic renal cell carcinoma.Transl Cancer Res. 2019 Dec;8(8):E1-E6. doi: 10.21037/tcr.2019.07.02. Transl Cancer Res. 2019. PMID: 35117054 Free PMC article. No abstract available.
-
Avelumab plus axitinib vs. sunitinib for advanced renal-cell carcinoma.Transl Cancer Res. 2019 Dec;8(Suppl 6):S585-S588. doi: 10.21037/tcr.2019.06.39. Transl Cancer Res. 2019. PMID: 35117136 Free PMC article. No abstract available.
Similar articles
-
Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma.N Engl J Med. 2019 Mar 21;380(12):1116-1127. doi: 10.1056/NEJMoa1816714. Epub 2019 Feb 16. N Engl J Med. 2019. PMID: 30779529 Clinical Trial.
-
Preliminary results for avelumab plus axitinib as first-line therapy in patients with advanced clear-cell renal-cell carcinoma (JAVELIN Renal 100): an open-label, dose-finding and dose-expansion, phase 1b trial.Lancet Oncol. 2018 Apr;19(4):451-460. doi: 10.1016/S1470-2045(18)30107-4. Epub 2018 Mar 9. Lancet Oncol. 2018. PMID: 29530667 Clinical Trial.
-
Updated efficacy results from the JAVELIN Renal 101 trial: first-line avelumab plus axitinib versus sunitinib in patients with advanced renal cell carcinoma.Ann Oncol. 2020 Aug;31(8):1030-1039. doi: 10.1016/j.annonc.2020.04.010. Epub 2020 Apr 25. Ann Oncol. 2020. PMID: 32339648 Free PMC article. Clinical Trial.
-
Avelumab and axitinib in the treatment of renal cell carcinoma: safety and efficacy.Expert Rev Anticancer Ther. 2020 May;20(5):343-354. doi: 10.1080/14737140.2020.1756780. Epub 2020 May 7. Expert Rev Anticancer Ther. 2020. PMID: 32293937 Review.
-
[Risk-adapted therapy for metastatic renal cell carcinoma].Urologe A. 2020 Feb;59(2):155-161. doi: 10.1007/s00120-020-01131-x. Urologe A. 2020. PMID: 32006060 Review. German.
Cited by
-
A Multi-Omics Prognostic Model Capturing Tumor Stemness and the Immune Microenvironment in Clear Cell Renal Cell Carcinoma.Biomedicines. 2024 Sep 24;12(10):2171. doi: 10.3390/biomedicines12102171. Biomedicines. 2024. PMID: 39457484 Free PMC article.
-
Systemic therapy for advanced clear cell renal cell carcinoma after discontinuation of immune-oncology and VEGF targeted therapy combinations.BMC Urol. 2020 Jul 2;20(1):84. doi: 10.1186/s12894-020-00647-w. BMC Urol. 2020. PMID: 32616076 Free PMC article.
-
Small-molecule inhibitors, immune checkpoint inhibitors, and more: FDA-approved novel therapeutic drugs for solid tumors from 1991 to 2021.J Hematol Oncol. 2022 Oct 8;15(1):143. doi: 10.1186/s13045-022-01362-9. J Hematol Oncol. 2022. PMID: 36209184 Free PMC article. Review.
-
Current status of antigen-specific T-cell immunotherapy for advanced renal-cell carcinoma.Hum Vaccin Immunother. 2021 Jul 3;17(7):1882-1896. doi: 10.1080/21645515.2020.1870846. Epub 2021 Mar 5. Hum Vaccin Immunother. 2021. PMID: 33667140 Free PMC article. Review.
-
Proliferative potential and response to nivolumab in clear cell renal cell carcinoma patients.Oncoimmunology. 2020 Jun 10;9(1):1773200. doi: 10.1080/2162402X.2020.1773200. Oncoimmunology. 2020. PMID: 32923131 Free PMC article.
References
-
- American Cancer Society. Survival rates for kidney cancer by stage. 2017. (https://www.cancer.org/cancer/kidney-cancer/detection-diagnosis-staging/...).
-
- Choueiri TK, Motzer RJ. Systemic therapy for metastatic renal-cell carcinoma. N Engl J Med 2017;376:354–66. - PubMed
-
- National Comprehensive Cancer Net-work. NCCN guidelines: kidney cancer. 2018. (https://www.nccn.org/professionals/physician_gls/PDF/kidney.pdf).
-
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med 2007;356:115–24. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials