

Global, regional, and national burden of epilepsy, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016
- PMID: 30773428
- PMCID: PMC6416168
- DOI: 10.1016/S1474-4422(18)30454-X
Global, regional, and national burden of epilepsy, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016
Erratum in
-
Correction to Lancet Neurol 2019; 18: 357-75.Lancet Neurol. 2019 May;18(5):e4. doi: 10.1016/S1474-4422(19)30120-6. Lancet Neurol. 2019. PMID: 30981323 Free PMC article. No abstract available.
Abstract
Background: Seizures and their consequences contribute to the burden of epilepsy because they can cause health loss (premature mortality and residual disability). Data on the burden of epilepsy are needed for health-care planning and resource allocation. The aim of this study was to quantify health loss due to epilepsy by age, sex, year, and location using data from the Global Burden of Diseases, Injuries, and Risk Factors Study.
Methods: We assessed the burden of epilepsy in 195 countries and territories from 1990 to 2016. Burden was measured as deaths, prevalence, and disability-adjusted life-years (DALYs; a summary measure of health loss defined by the sum of years of life lost [YLLs] for premature mortality and years lived with disability), by age, sex, year, location, and Socio-demographic Index (SDI; a compound measure of income per capita, education, and fertility). Vital registrations and verbal autopsies provided information about deaths, and data on the prevalence and severity of epilepsy largely came from population representative surveys. All estimates were calculated with 95% uncertainty intervals (UIs).
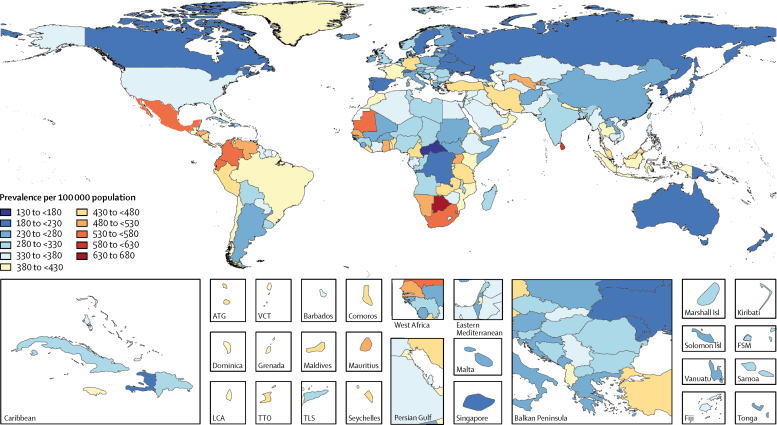
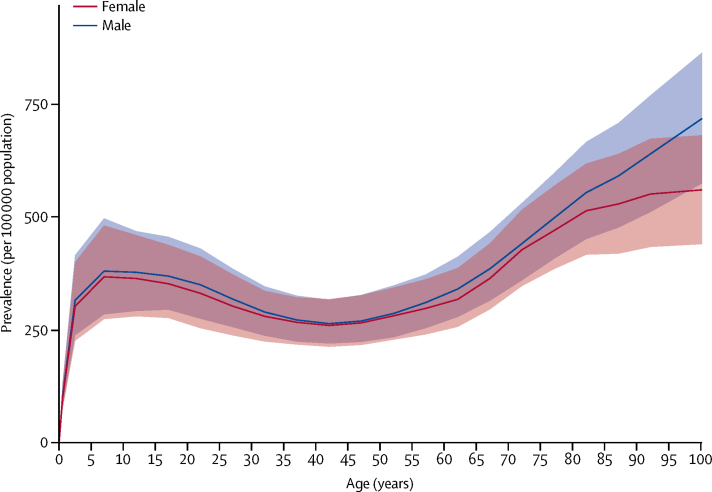
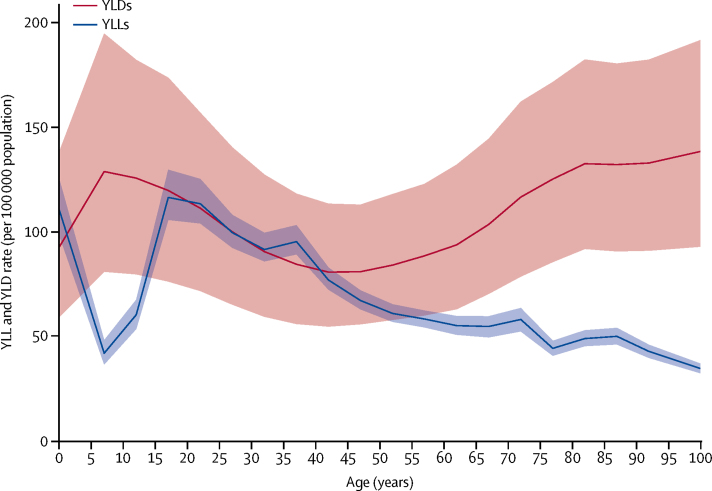
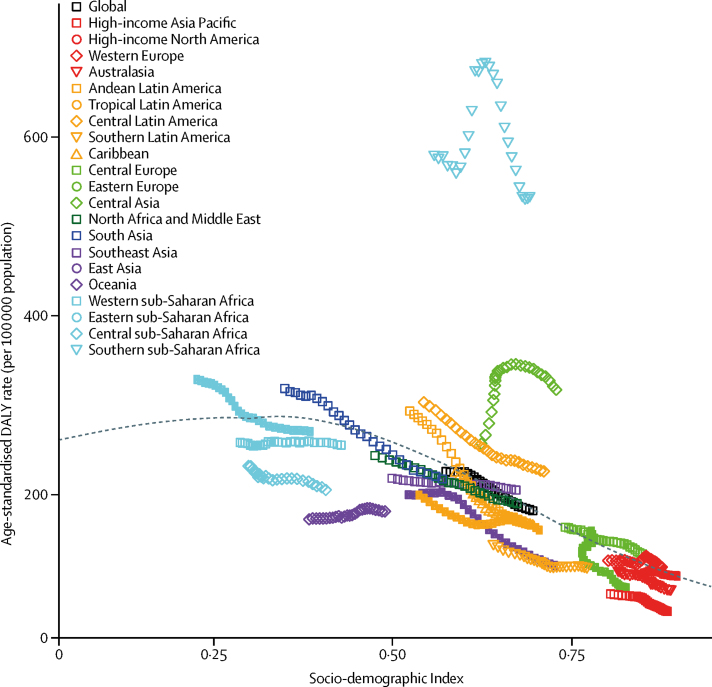
Findings: In 2016, there were 45·9 million (95% UI 39·9-54·6) patients with all-active epilepsy (both idiopathic and secondary epilepsy globally; age-standardised prevalence 621·5 per 100 000 population; 540·1-737·0). Of these patients, 24·0 million (20·4-27·7) had active idiopathic epilepsy (prevalence 326·7 per 100 000 population; 278·4-378·1). Prevalence of active epilepsy increased with age, with peaks at 5-9 years (374·8 [280·1-490·0]) and at older than 80 years of age (545·1 [444·2-652·0]). Age-standardised prevalence of active idiopathic epilepsy was 329·3 per 100 000 population (280·3-381·2) in men and 318·9 per 100 000 population (271·1-369·4) in women, and was similar among SDI quintiles. Global age-standardised mortality rates of idiopathic epilepsy were 1·74 per 100 000 population (1·64-1·87; 1·40 per 100 000 population [1·23-1·54] for women and 2·09 per 100 000 population [1·96-2·25] for men). Age-standardised DALYs were 182·6 per 100 000 population (149·0-223·5; 163·6 per 100 000 population [130·6-204·3] for women and 201·2 per 100 000 population [166·9-241·4] for men). The higher DALY rates in men were due to higher YLL rates compared with women. Between 1990 and 2016, there was a non-significant 6·0% (-4·0 to 16·7) change in the age-standardised prevalence of idiopathic epilepsy, but a significant decrease in age-standardised mortality rates (24·5% [10·8 to 31·8]) and age-standardised DALY rates (19·4% [9·0 to 27·6]). A third of the difference in age-standardised DALY rates between low and high SDI quintile countries was due to the greater severity of epilepsy in low-income settings, and two-thirds were due to a higher YLL rate in low SDI countries.
Interpretation: Despite the decrease in the disease burden from 1990 to 2016, epilepsy is still an important cause of disability and mortality. Standardised collection of data on epilepsy in population representative surveys will strengthen the estimates, particularly in countries for which we currently have no or sparse data and if additional data is collected on severity, causes, and treatment. Sizeable gains in reducing the burden of epilepsy might be expected from improved access to existing treatments in low-income countries and from the development of new effective drugs worldwide.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
An unparalleled assessment of the global burden of epilepsy.Lancet Neurol. 2019 Apr;18(4):322-324. doi: 10.1016/S1474-4422(19)30042-0. Epub 2019 Feb 14. Lancet Neurol. 2019. PMID: 30773429 No abstract available.
Similar articles
-
Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021.Lancet. 2024 May 18;403(10440):2133-2161. doi: 10.1016/S0140-6736(24)00757-8. Epub 2024 Apr 17. Lancet. 2024. PMID: 38642570 Free PMC article.
-
Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016.Lancet. 2017 Sep 16;390(10100):1151-1210. doi: 10.1016/S0140-6736(17)32152-9. Lancet. 2017. PMID: 28919116 Free PMC article.
-
Global, regional, and national burden of brain and other CNS cancer, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016.Lancet Neurol. 2019 Apr;18(4):376-393. doi: 10.1016/S1474-4422(18)30468-X. Epub 2019 Feb 21. Lancet Neurol. 2019. PMID: 30797715 Free PMC article.
-
Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010.Lancet. 2013 Nov 9;382(9904):1575-86. doi: 10.1016/S0140-6736(13)61611-6. Epub 2013 Aug 29. Lancet. 2013. PMID: 23993280 Review.
-
Global burden of disease attributable to illicit drug use and dependence: findings from the Global Burden of Disease Study 2010.Lancet. 2013 Nov 9;382(9904):1564-74. doi: 10.1016/S0140-6736(13)61530-5. Epub 2013 Aug 29. Lancet. 2013. PMID: 23993281 Review.
Cited by
-
Characteristics of people with epilepsy in three Eastern African countries - a pooled analysis.BMC Neurol. 2022 Aug 26;22(1):321. doi: 10.1186/s12883-022-02813-z. BMC Neurol. 2022. PMID: 36028820 Free PMC article.
-
Behavioral and Molecular Responses to Exogenous Cannabinoids During Pentylenetetrazol-Induced Convulsions in Male and Female Rats.Front Mol Neurosci. 2022 Aug 9;15:868583. doi: 10.3389/fnmol.2022.868583. eCollection 2022. Front Mol Neurosci. 2022. PMID: 36147210 Free PMC article.
-
Targeted suppression of mTORC2 reduces seizures across models of epilepsy.Nat Commun. 2023 Nov 14;14(1):7364. doi: 10.1038/s41467-023-42922-y. Nat Commun. 2023. PMID: 37963879 Free PMC article.
-
Educational inequalities in epilepsy mortality in the Baltic countries and Finland in 2000-2015.Sci Rep. 2022 Mar 17;12(1):4597. doi: 10.1038/s41598-022-08456-x. Sci Rep. 2022. PMID: 35301362 Free PMC article.
-
PET/MRI in the Presurgical Evaluation of Patients with Epilepsy: A Concordance Analysis.Biomedicines. 2022 Apr 20;10(5):949. doi: 10.3390/biomedicines10050949. Biomedicines. 2022. PMID: 35625684 Free PMC article.
References
-
- Neligan A, Hauser WA, Sander JW. The epidemiology of the epilepsies. Handb Clin Neurol. 2012;107:113–133. - PubMed
-
- Fisher RS, Cross JH, French JA. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58:522–530. - PubMed
-
- Newton CR, Garcia HH. Epilepsy in poor regions of the world. Lancet. 2012;380:1193–1201. - PubMed
-
- Beghi E, Giussani G, Sander JW. The natural history and prognosis of epilepsy. Epileptic Disord. 2015;17:243–253. - PubMed
-
- WHO . World Health Organization; Geneva: 2006. Neurological disorders: public health challenges.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
