

Sepsis Surveillance Using Adult Sepsis Events Simplified eSOFA Criteria Versus Sepsis-3 Sequential Organ Failure Assessment Criteria
- PMID: 30768498
- PMCID: PMC6383796
- DOI: 10.1097/CCM.0000000000003521
Sepsis Surveillance Using Adult Sepsis Events Simplified eSOFA Criteria Versus Sepsis-3 Sequential Organ Failure Assessment Criteria
Abstract
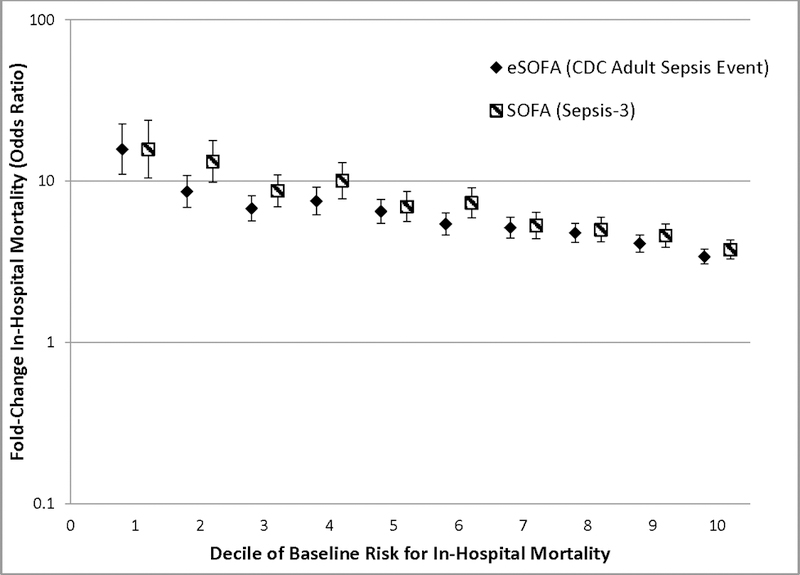
Objectives: Sepsis-3 defines organ dysfunction as an increase in the Sequential Organ Failure Assessment score by greater than or equal to 2 points. However, some Sequential Organ Failure Assessment score components are not routinely recorded in all hospitals' electronic health record systems, limiting its utility for wide-scale sepsis surveillance. The Centers for Disease Control and Prevention recently released the Adult Sepsis Event surveillance definition that includes simplified organ dysfunction criteria optimized for electronic health records (eSOFA). We compared eSOFA versus Sequential Organ Failure Assessment with regard to sepsis prevalence, overlap, and outcomes.
Design: Retrospective cohort study.
Setting: One hundred eleven U.S. hospitals in the Cerner HealthFacts dataset.
Patients: Adults hospitalized in 2013-2015.
Interventions: None.
Measurements and main results: We identified clinical indicators of presumed infection (blood cultures and antibiotics) concurrent with either: 1) an increase in Sequential Organ Failure Assessment score by 2 or more points (Sepsis-3) or 2) 1 or more eSOFA criteria: vasopressor initiation, mechanical ventilation initiation, lactate greater than or equal to 2.0 mmol/L, doubling in creatinine, doubling in bilirubin to greater than or equal to 2.0 mg/dL, or greater than or equal to 50% decrease in platelet count to less than 100 cells/μL (Centers for Disease Control and Prevention Adult Sepsis Event). We compared area under the receiver operating characteristic curves for discriminating in-hospital mortality, adjusting for baseline characteristics. Of 942,360 patients in the cohort, 57,242 (6.1%) had sepsis by Sequential Organ Failure Assessment versus 41,618 (4.4%) by eSOFA. Agreement between sepsis by Sequential Organ Failure Assessment and eSOFA was good (Cronbach's alpha 0.81). Baseline characteristics and infectious diagnoses were similar, but mortality was higher with eSOFA (17.1%) versus Sequential Organ Failure Assessment (14.4%; p < 0.001) as was discrimination for mortality (area under the receiver operating characteristic curve, 0.774 vs 0.759; p < 0.001). Comparisons were consistent across subgroups of age, infectious diagnoses, and comorbidities.
Conclusions: The Adult Sepsis Event's eSOFA organ dysfunction criteria identify a smaller, more severely ill sepsis cohort compared with the Sequential Organ Failure Assessment score, but with good overlap and similar clinical characteristics. Adult Sepsis Events may facilitate wide-scale automated sepsis surveillance that tracks closely with the more complex Sepsis-3 criteria.
Conflict of interest statement
Figures

Comment in
-
Surveillance for Adult Sepsis Events: An Idea Whose Time Has Come.Crit Care Med. 2019 Mar;47(3):467-468. doi: 10.1097/CCM.0000000000003561. Crit Care Med. 2019. PMID: 30768502 No abstract available.
Similar articles
-
External validity of Adult Sepsis Event's simplified eSOFA criteria: a retrospective analysis of patients with confirmed infection in China.Ann Intensive Care. 2020 Feb 4;10(1):14. doi: 10.1186/s13613-020-0629-1. Ann Intensive Care. 2020. PMID: 32020406 Free PMC article.
-
External validation and comparison of two versions of simplified sequential organ failure assessment scores to predict prognosis of septic patients.Int J Clin Pract. 2021 Dec;75(12):e14865. doi: 10.1111/ijcp.14865. Epub 2021 Sep 26. Int J Clin Pract. 2021. PMID: 34523203
-
Variation in Identifying Sepsis and Organ Dysfunction Using Administrative Versus Electronic Clinical Data and Impact on Hospital Outcome Comparisons.Crit Care Med. 2019 Apr;47(4):493-500. doi: 10.1097/CCM.0000000000003554. Crit Care Med. 2019. PMID: 30431493 Free PMC article.
-
The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).JAMA. 2016 Feb 23;315(8):801-10. doi: 10.1001/jama.2016.0287. JAMA. 2016. PMID: 26903338 Free PMC article.
-
Surveillance Strategies for Tracking Sepsis Incidence and Outcomes.J Infect Dis. 2020 Jul 21;222(Suppl 2):S74-S83. doi: 10.1093/infdis/jiaa102. J Infect Dis. 2020. PMID: 32691830 Free PMC article. Review.
Cited by
-
Evaluating Pediatric Sepsis Definitions Designed for Electronic Health Record Extraction and Multicenter Quality Improvement.Crit Care Med. 2020 Oct;48(10):e916-e926. doi: 10.1097/CCM.0000000000004505. Crit Care Med. 2020. PMID: 32931197 Free PMC article.
-
Association of Unit Census with Delays in Antimicrobial Initiation among Ward Patients with Hospital-acquired Sepsis.Ann Am Thorac Soc. 2022 Sep;19(9):1525-1533. doi: 10.1513/AnnalsATS.202112-1360OC. Ann Am Thorac Soc. 2022. PMID: 35312462 Free PMC article.
-
External validity of Adult Sepsis Event's simplified eSOFA criteria: a retrospective analysis of patients with confirmed infection in China.Ann Intensive Care. 2020 Feb 4;10(1):14. doi: 10.1186/s13613-020-0629-1. Ann Intensive Care. 2020. PMID: 32020406 Free PMC article.
-
Epidemiology of Hospital-Onset Versus Community-Onset Sepsis in U.S. Hospitals and Association With Mortality: A Retrospective Analysis Using Electronic Clinical Data.Crit Care Med. 2019 Sep;47(9):1169-1176. doi: 10.1097/CCM.0000000000003817. Crit Care Med. 2019. PMID: 31135503 Free PMC article.
-
Validation of automated sepsis surveillance based on the Sepsis-3 clinical criteria against physician record review in a general hospital population: observational study using electronic health records data.BMJ Qual Saf. 2020 Sep;29(9):735-745. doi: 10.1136/bmjqs-2019-010123. Epub 2020 Feb 6. BMJ Qual Saf. 2020. PMID: 32029574 Free PMC article.
References
-
- Vincent JL, Moreno R, Takala J et al.: The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996, 22(7):707–710. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
