

Vitamin D Status and Mortality: A Systematic Review of Observational Studies
- PMID: 30700025
- PMCID: PMC6388383
- DOI: 10.3390/ijerph16030383
Vitamin D Status and Mortality: A Systematic Review of Observational Studies
Abstract
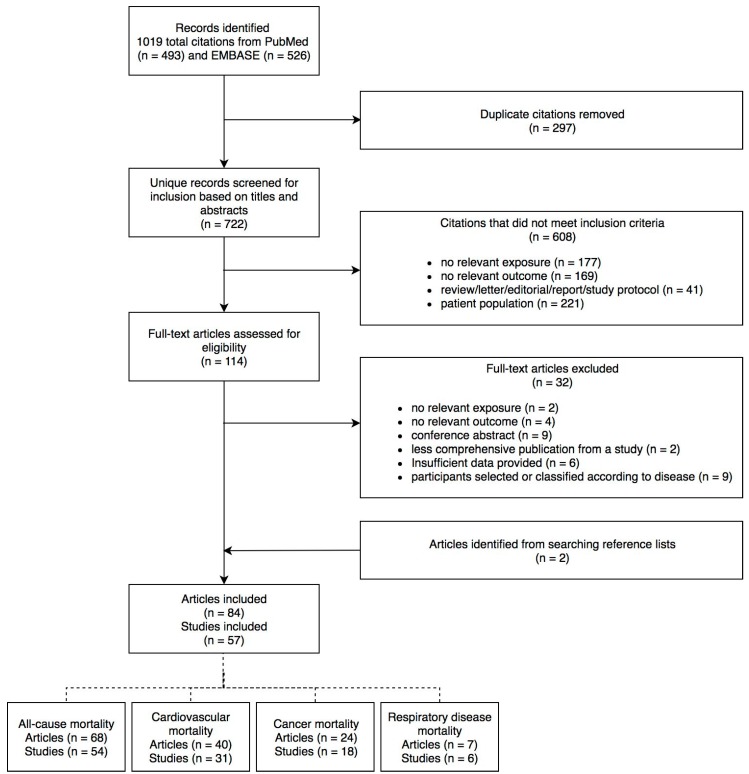
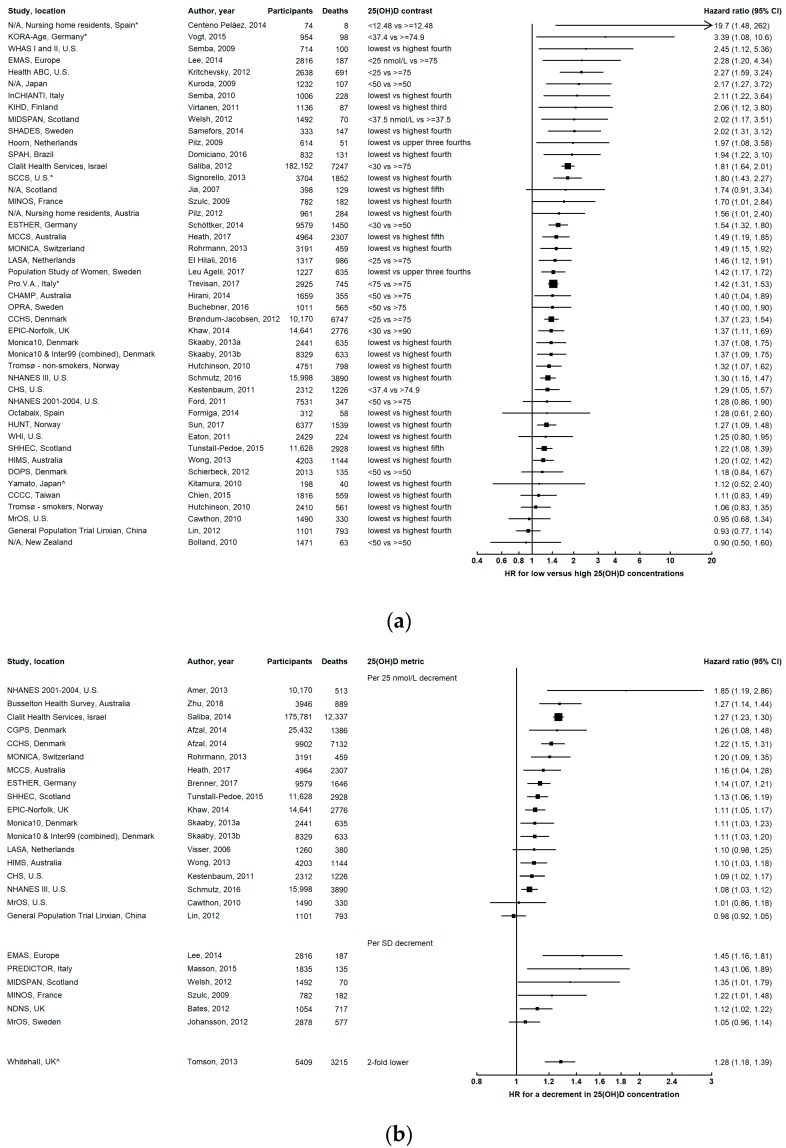
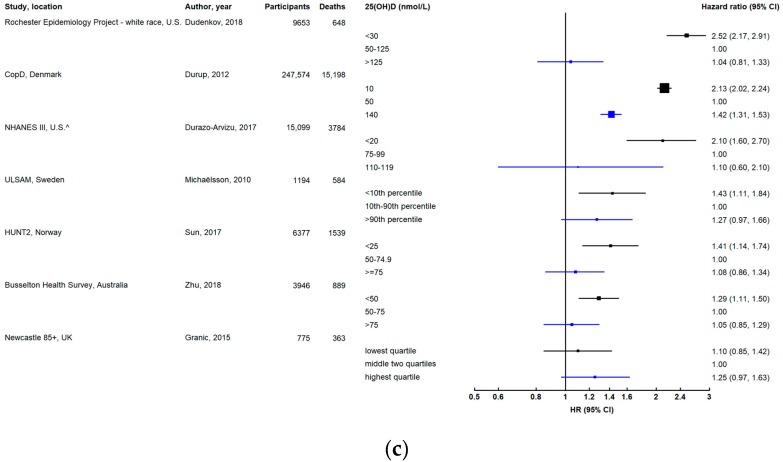
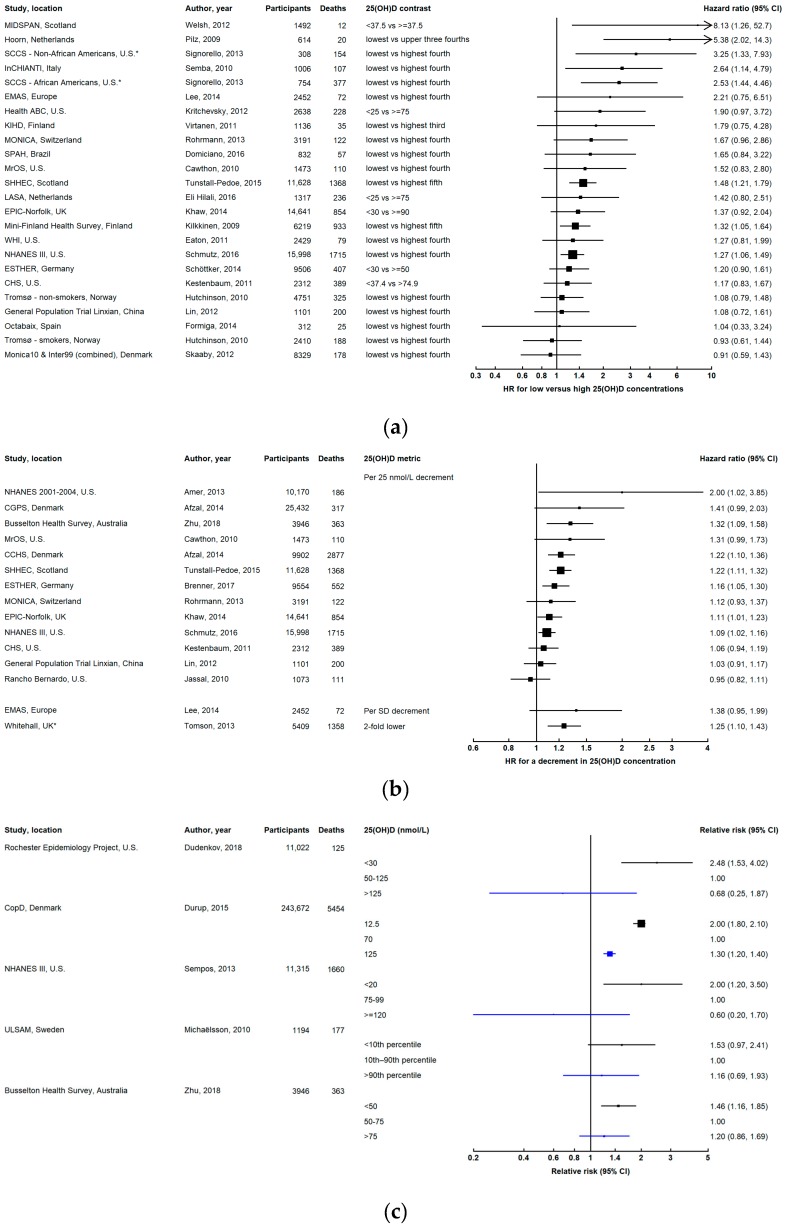
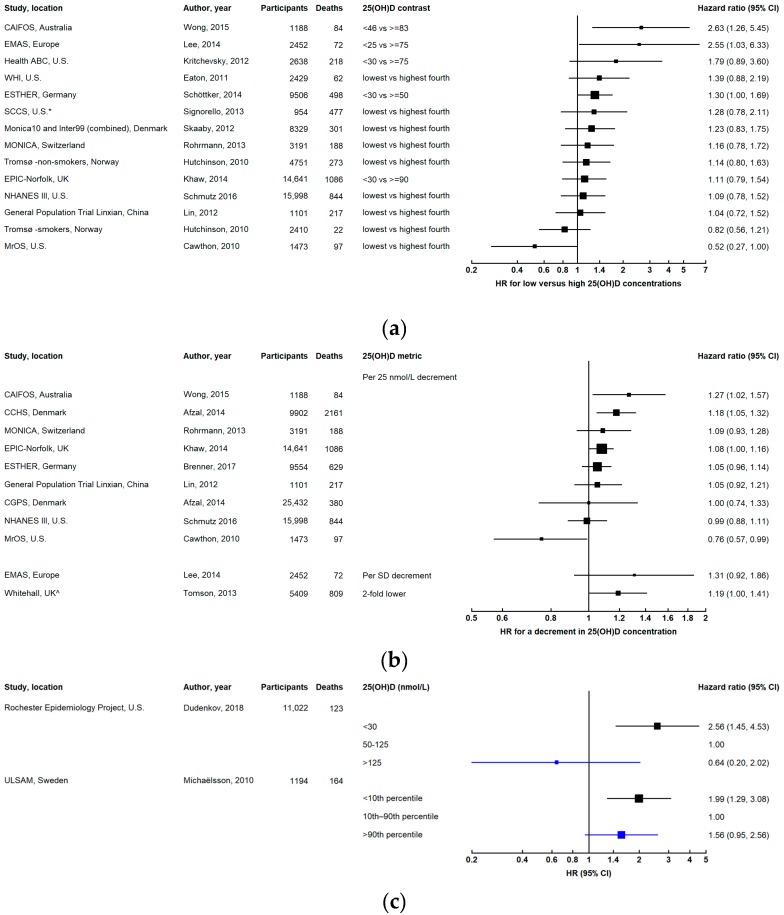
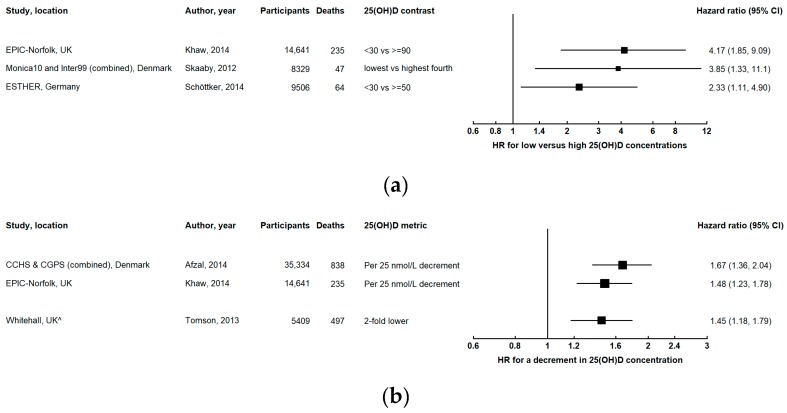
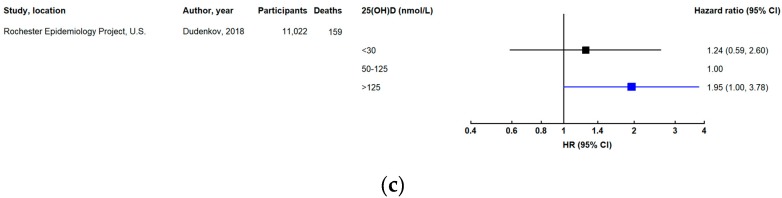
Epidemiological evidence suggests that vitamin D deficiency is associated with increased mortality, but it is unclear whether this is explained by reverse causation, and if there are specific causes of death for which vitamin D might be important. We conducted a systematic review of observational studies investigating associations between circulating 25-hydroxyvitamin D (25(OH)D) concentration and all-cause or cause-specific mortality in generally healthy populations. Relevant studies were identified using PubMed and EMBASE searches. After screening 722 unique records and removing those that were ineligible, 84 articles were included in this review. The vast majority of studies reported inverse associations between 25(OH)D concentration and all-cause mortality. This association appeared to be non-linear, with progressively lower mortality with increasing 25(OH)D up to a point, beyond which there was no further decrease. There is moderate evidence that vitamin D status is inversely associated with cancer mortality and death due to respiratory diseases, while for cardiovascular mortality, there is weak evidence of an association in observational studies, which is not supported by the data from intervention or Mendelian randomization studies. The relationship between vitamin D status and other causes of death remains uncertain due to limited data. Larger long-term studies are required to clarify these associations.
Keywords: 25-hydroxyvitamin D; all-cause mortality; cancer mortality; cardiovascular mortality; cause-specific mortality; mortality; respiratory disease mortality; systematic review; vitamin D; vitamin D status.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The relationship of vitamin D status to risk of cardiovascular disease and mortality.Dan Med J. 2015 Feb;62(2):B5008. Dan Med J. 2015. PMID: 25634511 Review.
-
Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies.BMJ. 2014 Apr 1;348:g1903. doi: 10.1136/bmj.g1903. BMJ. 2014. PMID: 24690623 Free PMC article. Review.
-
Vitamin D status and mortality risk among patients on dialysis: a systematic review and meta-analysis of observational studies.Nephrol Dial Transplant. 2018 Oct 1;33(10):1742-1751. doi: 10.1093/ndt/gfy016. Nephrol Dial Transplant. 2018. PMID: 29481620
-
Screening for Vitamin D Deficiency in Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force.JAMA. 2021 Apr 13;325(14):1443-1463. doi: 10.1001/jama.2020.26498. JAMA. 2021. PMID: 33847712
-
The inverse association between serum 25-hydroxyvitamin D and mortality may be modified by vitamin A status and use of vitamin A supplements.Eur J Nutr. 2016 Feb;55(1):393-402. doi: 10.1007/s00394-015-0860-y. Epub 2015 Feb 21. Eur J Nutr. 2016. PMID: 25701092
Cited by
-
Vitamin D-Binding Protein, Bioavailable, and Free 25(OH)D, and Mortality: A Systematic Review and Meta-Analysis.Nutrients. 2022 Sep 20;14(19):3894. doi: 10.3390/nu14193894. Nutrients. 2022. PMID: 36235547 Free PMC article. Review.
-
Additive effects of obesity and vitamin D insufficiency on all-cause and cause-specific mortality.Front Nutr. 2022 Oct 21;9:999489. doi: 10.3389/fnut.2022.999489. eCollection 2022. Front Nutr. 2022. PMID: 36337642 Free PMC article.
-
Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses.Lancet Diabetes Endocrinol. 2021 Dec;9(12):837-846. doi: 10.1016/S2213-8587(21)00263-1. Epub 2021 Oct 28. Lancet Diabetes Endocrinol. 2021. Retraction in: Lancet Diabetes Endocrinol. 2024 Jan;12(1):8. doi: 10.1016/S2213-8587(23)00364-9 Retracted and republished in: Lancet Diabetes Endocrinol. 2024 Jan;12(1):e2-e11. doi: 10.1016/S2213-8587(23)00287-5 PMID: 34717822 Free PMC article. Retracted. Retracted and republished.
-
Plasma 25-Hydroxyvitamin D Levels and VDR Gene Expression in Peripheral Blood Mononuclear Cells of Leukemia Patients and Healthy Subjects in Central Kazakhstan.Nutrients. 2020 Apr 26;12(5):1229. doi: 10.3390/nu12051229. Nutrients. 2020. PMID: 32357551 Free PMC article.
-
Therapeutic and prognostic role of vitamin D for COVID-19 infection: A systematic review and meta-analysis of 43 observational studies.J Steroid Biochem Mol Biol. 2021 Jul;211:105883. doi: 10.1016/j.jsbmb.2021.105883. Epub 2021 Mar 26. J Steroid Biochem Mol Biol. 2021. PMID: 33775818 Free PMC article.
References
-
- Chowdhury R., Kunutsor S., Vitezova A., Oliver-Williams C., Chowdhury S., Kiefte-de-Jong J.C., Khan H., Baena C.P., Prabhakaran D., Hoshen M.B., et al. Vitamin D and risk of cause specific death: Systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ. 2014;348:g1903. doi: 10.1136/bmj.g1903. - DOI - PMC - PubMed
-
- Garland C.F., Kim J.J., Mohr S.B., Gorham E.D., Grant W.B., Giovannucci E.L., Baggerly L., Hofflich H., Ramsdell J.W., Zeng K., et al. Meta-analysis of all-cause mortality according to serum 25-hydroxyvitamin D. Am. J. Public Health. 2014;104:e43–e50. doi: 10.2105/AJPH.2014.302034. - DOI - PMC - PubMed
-
- Gaksch M., Jorde R., Grimnes G., Joakimsen R., Schirmer H., Wilsgaard T., Mathiesen E.B., Njolstad I., Lochen M.L., Marz W., et al. Vitamin D and mortality: Individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS ONE. 2017;12:e0170791. doi: 10.1371/journal.pone.0170791. - DOI - PMC - PubMed
-
- Schöttker B., Jorde R., Peasey A., Thorand B., Jansen E.H., Groot L., Streppel M., Gardiner J., Ordóñez-Mena J.M., Perna L., et al. Vitamin D and mortality: Meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States. BMJ. 2014;348:g3656. doi: 10.1136/bmj.g3656. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
