

Recent advances in understanding and managing rosacea
- PMID: 30631431
- PMCID: PMC6281021
- DOI: 10.12688/f1000research.16537.1
Recent advances in understanding and managing rosacea
Abstract
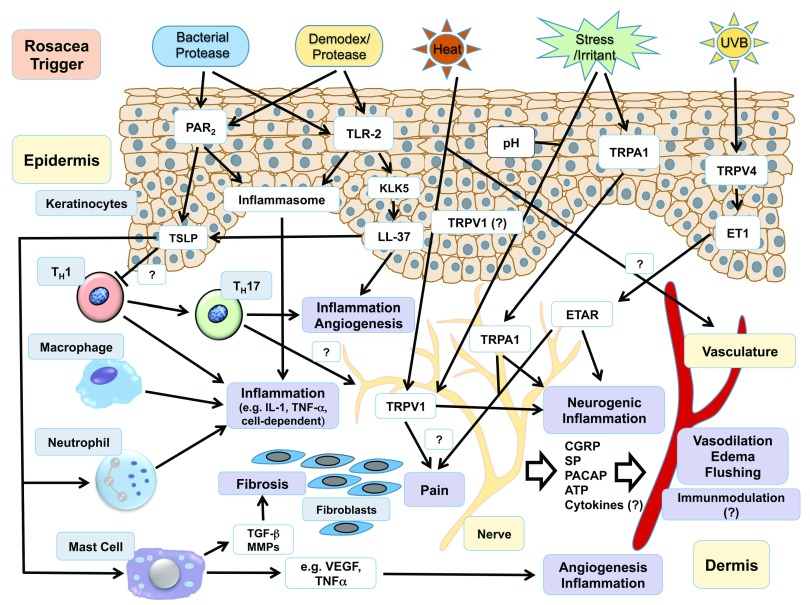
Rosacea is a common chronic inflammatory skin disease of the central facial skin and is of unknown origin. Currently, two classifications of rosacea exist that are based on either "preformed" clinical subtypes (erythematotelangiectatic, papulopustular, phymatous, and ocular) or patient-tailored analysis of the presented rosacea phenotype. Rosacea etiology and pathophysiology are poorly understood. However, recent findings indicate that genetic and environmental components can trigger rosacea initiation and aggravation by dysregulation of the innate and adaptive immune system. Trigger factors also lead to the release of various mediators such as keratinocytes (for example, cathelicidin, vascular endothelial growth factor, and endothelin-1), endothelial cells (nitric oxide), mast cells (cathelicidin and matrix metalloproteinases), macrophages (interferon-gamma, tumor necrosis factor, matrix metalloproteinases, and interleukin-26), and T helper type 1 (T H1) and T H17 cells. Additionally, trigger factors can directly communicate to the cutaneous nervous system and, by neurovascular and neuro-immune active neuropeptides, lead to the manifestation of rosacea lesions. Here, we aim to summarize the recent advances that preceded the new rosacea classification and address a symptom-based approach in the management of patients with rosacea.
Keywords: Cathelicidin; Classification; Immunity; Inflammation; Pathophysiology; Rosacea; Therapy.
Conflict of interest statement
No competing interests were disclosed.No competing interests were disclosed.No competing interests were disclosed.Competing interests: This reviewer has received support from Galderma.
Figures
Similar articles
-
New insights into rosacea pathophysiology: a review of recent findings.J Am Acad Dermatol. 2013 Dec;69(6 Suppl 1):S15-26. doi: 10.1016/j.jaad.2013.04.045. J Am Acad Dermatol. 2013. PMID: 24229632 Review.
-
Updates on the pathophysiology and management of acne rosacea.Postgrad Med. 2009 Sep;121(5):178-86. doi: 10.3810/pgm.2009.09.2066. Postgrad Med. 2009. PMID: 19820288 Review.
-
Rosacea: an update.Dermatology. 2005;210(2):100-8. doi: 10.1159/000082564. Dermatology. 2005. PMID: 15724091 Review.
-
Rosacea: part I. Introduction, categorization, histology, pathogenesis, and risk factors.J Am Acad Dermatol. 2015 May;72(5):749-58; quiz 759-60. doi: 10.1016/j.jaad.2014.08.028. J Am Acad Dermatol. 2015. PMID: 25890455 Review.
-
Rosacea: a review of current topical, systemic and light-based therapies.G Ital Dermatol Venereol. 2009 Dec;144(6):673-88. G Ital Dermatol Venereol. 2009. PMID: 19907406 Review.
Cited by
-
The Importance of Assessing Burning and Stinging when Managing Rosacea: A Review.Acta Derm Venereol. 2021 Oct 31;101(10):adv00584. doi: 10.2340/actadv.v101.356. Acta Derm Venereol. 2021. PMID: 34643244 Free PMC article. Review.
-
Efficacy and Safety of Microencapsulated Benzoyl Peroxide Cream, 5%, in Rosacea: Results From Two Phase III, Randomized, Vehicle-Controlled Trials.J Clin Aesthet Dermatol. 2023 Aug;16(8):34-40. J Clin Aesthet Dermatol. 2023. PMID: 37636253 Free PMC article.
-
The Effect of Capsaicin on Neuroinflammatory Mediators of Rosacea.Ann Dermatol. 2022 Aug;34(4):261-269. doi: 10.5021/ad.21.223. Ann Dermatol. 2022. PMID: 35948328 Free PMC article.
-
A Review of Systemic Minocycline Side Effects and Topical Minocycline as a Safer Alternative for Treating Acne and Rosacea.Antibiotics (Basel). 2021 Jun 22;10(7):757. doi: 10.3390/antibiotics10070757. Antibiotics (Basel). 2021. PMID: 34206485 Free PMC article. Review.
-
Recent Advances in the Management of Rosacea through Natural Compounds.Pharmaceuticals (Basel). 2024 Feb 6;17(2):212. doi: 10.3390/ph17020212. Pharmaceuticals (Basel). 2024. PMID: 38399428 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical