

Treatment of infantile spasms
- PMID: 30564773
- PMCID: PMC6293071
- DOI: 10.1002/epi4.12264
Treatment of infantile spasms
Abstract
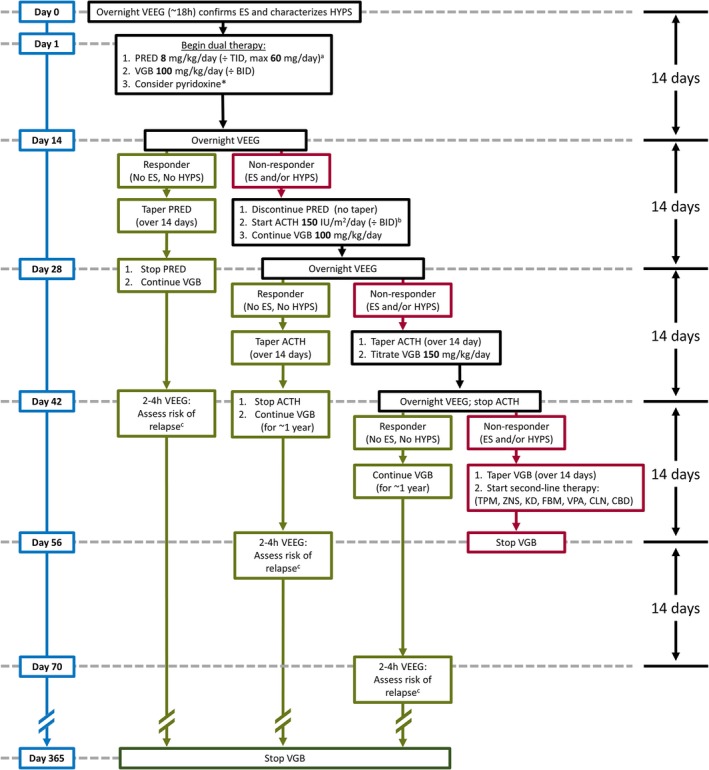
The treatment of infantile spasms is challenging, especially in the context of the following: (1) a severe phenotype with high morbidity and mortality; (2) the urgency of diagnosis and successful early response to therapy; and (3) the paucity of effective, safe, and well-tolerated therapies. Even after initially successful treatment, relapse risk is substantial and the most effective therapies pose considerable risk with long-term administration. In evaluating any treatment for infantile spasms, the key short-term outcome measure is freedom from both epileptic spasms and hypsarrhythmia. In contrast, the most important long-term outcomes are enduring seizure-freedom and measures of intellectual performance in later childhood and adulthood. First-line treatment options-namely hormonal therapy and vigabatrin-display moderate to high efficacy but also exhibit substantial side-effect burdens. Data on efficacy and safety of each class of therapy, as well as the combination of these therapies, are reviewed in detail. Specific hormonal therapies (adrenocorticotropic hormone and various corticosteroids) are contrasted. Those etiologies that prompt specific therapies are reviewed briefly, as are an array of second-line therapies supported by less-compelling data. The ketogenic diet is discussed in greater detail, with a focus on the limitations of numerous available studies that generally suggest that it is efficacious. Special discussion is allocated to cannabidiol-the investigational therapy that has received the most attention, and which is already in use in the form of various artisanal cannabis extracts. Finally, a treatment algorithm reflecting the concepts and controversies discussed in this review is presented.
Keywords: Epileptic encephalopathy; Epileptic spasms; Hypsarrhythmia; West syndrome.
Figures
Similar articles
-
Infantile Spasms: Outcome in Clinical Studies.Pediatr Neurol. 2020 Jul;108:54-64. doi: 10.1016/j.pediatrneurol.2020.01.015. Epub 2020 Feb 4. Pediatr Neurol. 2020. PMID: 32305143 Review.
-
Management of infantile spasms.Transl Pediatr. 2015 Oct;4(4):260-70. doi: 10.3978/j.issn.2224-4336.2015.09.01. Transl Pediatr. 2015. PMID: 26835388 Free PMC article. Review.
-
Adrenocorticotropic hormone for the treatment of West Syndrome in children.Ann Pharmacother. 2013 May;47(5):744-54. doi: 10.1345/aph.1R535. Epub 2013 Apr 19. Ann Pharmacother. 2013. PMID: 23606552 Review.
-
Safety and efficacy of vigabatrin for the treatment of infantile spasms.J Cent Nerv Syst Dis. 2011 Sep 14;3:199-207. doi: 10.4137/JCNSD.S6371. Print 2011. J Cent Nerv Syst Dis. 2011. PMID: 23861649 Free PMC article.
-
Long-term outcomes of infantile spasms in children treated with ketogenic diet therapy in combination with anti-seizure medications in a resource-limited region.Front Epidemiol. 2023 Jan 16;2:1080068. doi: 10.3389/fepid.2022.1080068. eCollection 2022. Front Epidemiol. 2023. PMID: 38455303 Free PMC article.
Cited by
-
Inequities in Therapy for Infantile Spasms: A Call to Action.Ann Neurol. 2022 Jul;92(1):32-44. doi: 10.1002/ana.26363. Epub 2022 Apr 28. Ann Neurol. 2022. PMID: 35388521 Free PMC article.
-
Modeling epileptic spasms during infancy: Are we heading for the treatment yet?Pharmacol Ther. 2020 Aug;212:107578. doi: 10.1016/j.pharmthera.2020.107578. Epub 2020 May 15. Pharmacol Ther. 2020. PMID: 32417271 Free PMC article. Review.
-
Limited efficacy of zonisamide in the treatment of refractory infantile spasms.Epilepsia Open. 2020 Jan 24;5(1):121-126. doi: 10.1002/epi4.12381. eCollection 2020 Mar. Epilepsia Open. 2020. PMID: 32140650 Free PMC article.
-
Compliance With Standard Therapies and Remission Rates After Implementation of an Infantile Spasms Management Guideline.Pediatr Neurol. 2020 Mar;104:23-29. doi: 10.1016/j.pediatrneurol.2019.11.016. Epub 2019 Dec 3. Pediatr Neurol. 2020. PMID: 31911027 Free PMC article.
-
Trends and Costs Associated With the Diagnosis and Treatment of Infantile Spasms: A 10-Year Multicenter Retrospective Review.J Pediatr Pharmacol Ther. 2022;27(1):29-37. doi: 10.5863/1551-6776-27.1.29. Epub 2021 Dec 22. J Pediatr Pharmacol Ther. 2022. PMID: 35002556 Free PMC article.
References
-
- Fisher RS, Cross JH, French JA, et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017;58:522–530. - PubMed
-
- Hrachovy RA, Frost JD, Kellaway P. Hypsarrhythmia: variations on the theme. Epilepsia 1984;25:317–325. - PubMed
-
- Caraballo RH, Fortini S, Reyes G, et al. Epileptic spasms in clusters and associated syndromes other than West syndrome: a study of 48 patients. Epilepsy Res 2016;123:29–35. - PubMed
-
- Gaily E, Lommi M, Lapatto R, et al. Incidence and outcome of epilepsy syndromes with onset in the first year of life: a retrospective population‐based study. Epilepsia 2016;57:1594–1601. - PubMed
-
- Hussain SA, Lay J, Cheng E, et al. Recognition of infantile spasms is often delayed: the ASSIST study. J Pediatr 2017;190:215–221. - PubMed
LinkOut - more resources
Full Text Sources
