

Body mass index and basal androstenedione are independent risk factors for miscarriage in polycystic ovary syndrome
- PMID: 30454060
- PMCID: PMC6245701
- DOI: 10.1186/s12958-018-0438-7
Body mass index and basal androstenedione are independent risk factors for miscarriage in polycystic ovary syndrome
Abstract
Background: There is limited literature investigating the effects of body mass index (BMI) and androgen level on in vitro fertilization (IVF) outcomes with a gonadotropin-releasing hormone (GnRH)-antagonist protocol in polycystic ovary syndrome (PCOS). Androgen-related variation in the effect of body mass index (BMI) on IVF outcomes remains unknown.
Methods: In this retrospective study, 583 infertile women with PCOS who underwent IVF using the conventional GnRH-antagonist protocol were included. Patients were divided into four groups according to BMI and androgen level: overweight- hyperandrogenism(HA) group, n = 96, overweight-non-HA group, n = 117, non-overweight-HA group, n = 152, and non-overweight-non-HA group, n = 218.
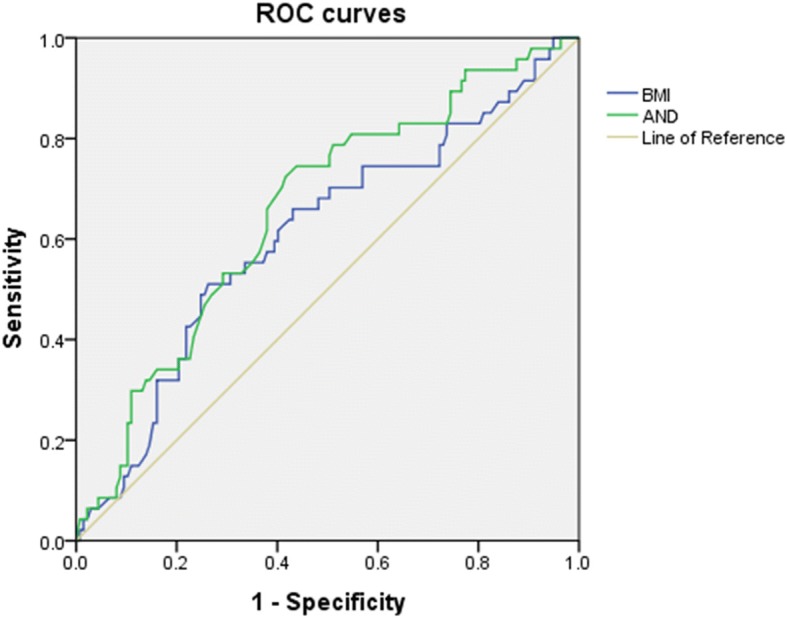
Results: A significantly higher number of oocytes were retrieved, and the total Gn consumption as well Gn consumption per day was significantly lower, in the non-overweight groups than in the overweight groups. The number of available embryos was significantly higher in the HA groups than in the non-HA groups. Clinical pregnancy rate was of no significant difference among four groups. Live-birth rates in the overweight groups were significantly lower than those in non-overweight-non-HA group (23.9, 28.4% vs. 42.5%, P<0.05). The miscarriage rate in overweight-HA group was significantly higher than that in non-overweight-non-HA group (45.2% vs. 14.5%, P<0.05). Multivariate logistic regression analysis revealed that BMI and basal androstenedione (AND) both acted as significantly influent factors on miscarriage rate. The area under the curve (AUC) in receiver operating characteristic (ROC) analysis for BMI and basal AND on miscarriage rate were 0.607 (P = 0.029) and 0.657 (P = 0.001), respectively, and the cut-off values of BMI and basal AND were 25.335 kg/m2 and 10.95 nmol/L, respectively.
Conclusions: In IVF cycles with GnRH-antagonist protocol, economic benefits were seen in non-overweight patients with PCOS, with less Gn cost and more retrieved oocytes. BMI and basal AND were both significantly influential factors with moderate predictive ability on the miscarriage rate. The predictive value of basal AND on miscarriage was slightly stronger than BMI.
Keywords: Body mass index; Gonadotropin-releasing hormone antagonist; Hyperandrogenism; In vitro fertilization; Polycystic ovary syndrome.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of the Department of Obstetrics and Gynecology, Peking University Third Hospital. Since this is a retrospective investigation, patients were not asked to participate in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Infertile polycystic ovary syndrome patients undergoing in vitro fertilization with the gonadotropin-releasing hormone-antagonist protocol: role of hyperandrogenism.Gynecol Endocrinol. 2018 Aug;34(8):715-718. doi: 10.1080/09513590.2018.1431773. Epub 2018 Jan 28. Gynecol Endocrinol. 2018. PMID: 29376451
-
In-vitro maturation of oocytes vs in-vitro fertilization with a gonadotropin-releasing hormone antagonist for women with polycystic ovarian syndrome: can superiority be defined?Eur J Obstet Gynecol Reprod Biol. 2014 Aug;179:46-50. doi: 10.1016/j.ejogrb.2014.05.013. Epub 2014 Jun 2. Eur J Obstet Gynecol Reprod Biol. 2014. PMID: 24965979
-
[Effect of hyperandrogenism on pregnancy outcomes in women with polycystic ovary syndrome undergoing in vitro fertilization/intracytoplasmic sperm injection-embryo transfer].Zhonghua Yi Xue Za Zhi. 2023 Apr 11;103(14):1042-1048. doi: 10.3760/cma.j.cn112137-20220926-02032. Zhonghua Yi Xue Za Zhi. 2023. PMID: 37032154 Chinese.
-
Effectiveness of GnRH antagonist in the treatment of patients with polycystic ovary syndrome undergoing IVF: a systematic review and meta analysis.Gynecol Endocrinol. 2013 Mar;29(3):187-91. doi: 10.3109/09513590.2012.736561. Epub 2012 Nov 30. Gynecol Endocrinol. 2013. PMID: 23194095 Review.
-
Management of women with PCOS using myo-inositol and folic acid. New clinical data and review of the literature.Horm Mol Biol Clin Investig. 2018 Mar 2;34(2):/j/hmbci.2018.34.issue-2/hmbci-2017-0067/hmbci-2017-0067.xml. doi: 10.1515/hmbci-2017-0067. Horm Mol Biol Clin Investig. 2018. PMID: 29498933 Review.
Cited by
-
The Effect of Ageing on Clinical, Hormonal and Sonographic Features Associated with PCOS-A Long-Term Follow-Up Study.J Clin Med. 2021 May 13;10(10):2101. doi: 10.3390/jcm10102101. J Clin Med. 2021. PMID: 34068234 Free PMC article.
-
Inflammation mediates the effect of adiposity and lipid metabolism indicators on the embryogenesis of PCOS women undergoing in vitro fertilization/intracytoplasmic sperm injection.Front Endocrinol (Lausanne). 2023 Jul 25;14:1198602. doi: 10.3389/fendo.2023.1198602. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37560312 Free PMC article.
-
Protective efficacy of dark chocolate in letrozole-induced ovary toxicity model rats: hormonal, biochemical, and histopathological investigation.J Tradit Chin Med. 2022 Oct;42(5):741-748. doi: 10.19852/j.cnki.jtcm.2022.05.007. J Tradit Chin Med. 2022. PMID: 36083481 Free PMC article.
-
Association between Pre-Pregnancy Overweightness/Obesity and Pregnancy Outcomes in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis.Int J Environ Res Public Health. 2022 Jul 26;19(15):9094. doi: 10.3390/ijerph19159094. Int J Environ Res Public Health. 2022. PMID: 35897496 Free PMC article.
-
Overweight and obesity determined by body mass index criteria for Asian populations adversely affect assisted reproductive outcomes among Chinese women with polycystic ovary syndrome.Int J Obes (Lond). 2024 Mar;48(3):394-402. doi: 10.1038/s41366-023-01430-1. Epub 2023 Dec 8. Int J Obes (Lond). 2024. PMID: 38066333
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
