

Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer
- PMID: 30415637
- PMCID: PMC6392053
- DOI: 10.1056/NEJMoa1811403
Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer
Abstract
Background: Higher intake of marine n-3 (also called omega-3) fatty acids has been associated with reduced risks of cardiovascular disease and cancer in several observational studies. Whether supplementation with n-3 fatty acids has such effects in general populations at usual risk for these end points is unclear.
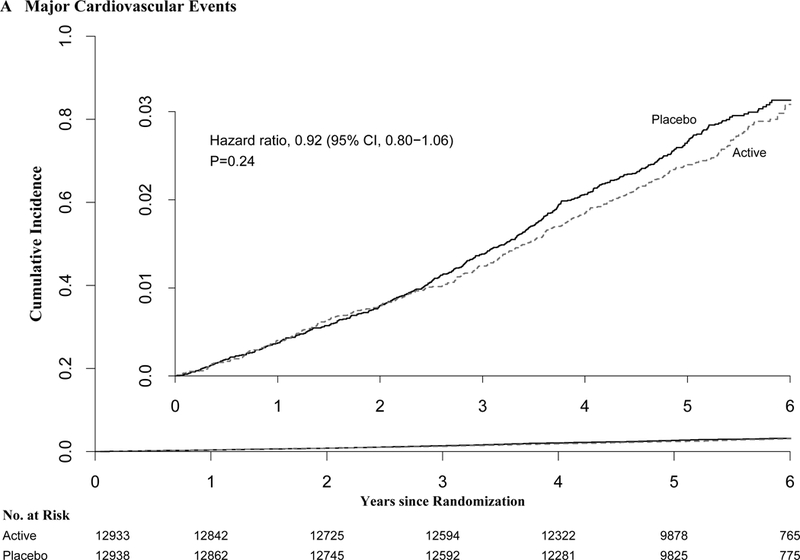
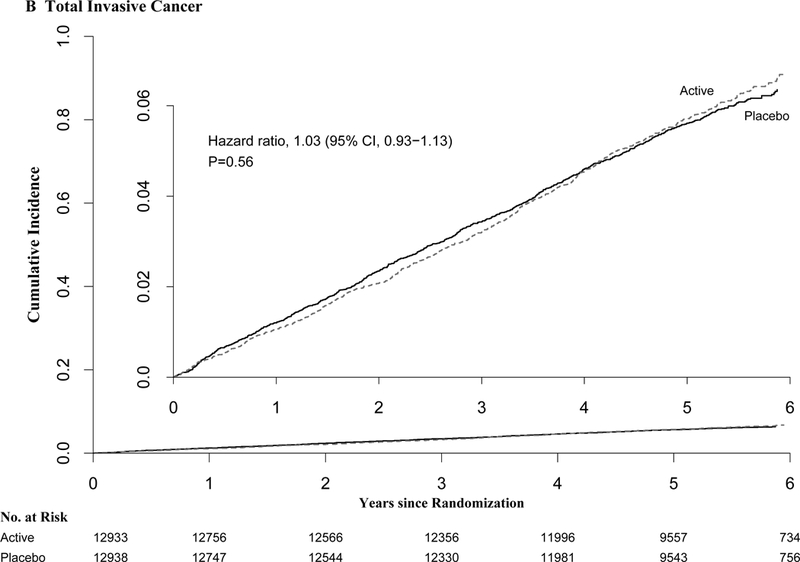
Methods: We conducted a randomized, placebo-controlled trial, with a two-by-two factorial design, of vitamin D3 (at a dose of 2000 IU per day) and marine n-3 fatty acids (at a dose of 1 g per day) in the primary prevention of cardiovascular disease and cancer among men 50 years of age or older and women 55 years of age or older in the United States. Primary end points were major cardiovascular events (a composite of myocardial infarction, stroke, or death from cardiovascular causes) and invasive cancer of any type. Secondary end points included individual components of the composite cardiovascular end point, the composite end point plus coronary revascularization (expanded composite of cardiovascular events), site-specific cancers, and death from cancer. Safety was also assessed. This article reports the results of the comparison of n-3 fatty acids with placebo.
Results: A total of 25,871 participants, including 5106 black participants, underwent randomization. During a median follow-up of 5.3 years, a major cardiovascular event occurred in 386 participants in the n-3 group and in 419 in the placebo group (hazard ratio, 0.92; 95% confidence interval [CI], 0.80 to 1.06; P=0.24). Invasive cancer was diagnosed in 820 participants in the n-3 group and in 797 in the placebo group (hazard ratio, 1.03; 95% CI, 0.93 to 1.13; P=0.56). In the analyses of key secondary end points, the hazard ratios were as follows: for the expanded composite end point of cardiovascular events, 0.93 (95% CI, 0.82 to 1.04); for total myocardial infarction, 0.72 (95% CI, 0.59 to 0.90); for total stroke, 1.04 (95% CI, 0.83 to 1.31); for death from cardiovascular causes, 0.96 (95% CI, 0.76 to 1.21); and for death from cancer (341 deaths from cancer), 0.97 (95% CI, 0.79 to 1.20). In the analysis of death from any cause (978 deaths overall), the hazard ratio was 1.02 (95% CI, 0.90 to 1.15). No excess risks of bleeding or other serious adverse events were observed.
Conclusions: Supplementation with n-3 fatty acids did not result in a lower incidence of major cardiovascular events or cancer than placebo. (Funded by the National Institutes of Health and others; VITAL ClinicalTrials.gov number, NCT01169259 .).
Conflict of interest statement
Figures
Comment in
-
VITAL Signs for Dietary Supplementation to Prevent Cancer and Heart Disease.N Engl J Med. 2019 Jan 3;380(1):91-93. doi: 10.1056/NEJMe1814933. Epub 2018 Nov 10. N Engl J Med. 2019. PMID: 30415594 No abstract available.
-
Dietary supplements undergo VITAL test.Nat Rev Cardiol. 2019 Jan;16(1):2-3. doi: 10.1038/s41569-018-0132-7. Nat Rev Cardiol. 2019. PMID: 30487541 No abstract available.
-
Vitamin D und Fischöl fallen beim Test durch.MMW Fortschr Med. 2019 Apr;161(6):33. doi: 10.1007/s15006-019-0349-3. MMW Fortschr Med. 2019. PMID: 30937778 Review. German. No abstract available.
-
VITAL study: an incomplete picture?Eur Rev Med Pharmacol Sci. 2019 Apr;23(7):3142-3147. doi: 10.26355/eurrev_201904_17599. Eur Rev Med Pharmacol Sci. 2019. PMID: 31002167 No abstract available.
-
Marine n-3 Fatty Acids and Vitamin D Supplementation and Primary Prevention.N Engl J Med. 2019 May 9;380(19):1878. doi: 10.1056/NEJMc1902636. N Engl J Med. 2019. PMID: 31067388 No abstract available.
-
Marine n-3 Fatty Acids and Vitamin D Supplementation and Primary Prevention.N Engl J Med. 2019 May 9;380(19):1878. doi: 10.1056/NEJMc1902636. N Engl J Med. 2019. PMID: 31067389 No abstract available.
-
Marine n-3 Fatty Acids and Vitamin D Supplementation and Primary Prevention.N Engl J Med. 2019 May 9;380(19):1878-1879. doi: 10.1056/NEJMc1902636. N Engl J Med. 2019. PMID: 31067390 No abstract available.
-
Marine n-3 Fatty Acids and Vitamin D Supplementation and Primary Prevention.N Engl J Med. 2019 May 9;380(19):1879. doi: 10.1056/NEJMc1902636. N Engl J Med. 2019. PMID: 31067391 No abstract available.
-
New Guidelines for Statistical Reporting in the Journal.N Engl J Med. 2019 Jul 18;381(3):285-286. doi: 10.1056/NEJMe1906559. N Engl J Med. 2019. PMID: 31314974 No abstract available.
Similar articles
-
Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease.N Engl J Med. 2019 Jan 3;380(1):33-44. doi: 10.1056/NEJMoa1809944. Epub 2018 Nov 10. N Engl J Med. 2019. PMID: 30415629 Free PMC article. Clinical Trial.
-
Vitamin D, Marine n-3 Fatty Acids, and Primary Prevention of Cardiovascular Disease Current Evidence.Circ Res. 2020 Jan 3;126(1):112-128. doi: 10.1161/CIRCRESAHA.119.314541. Epub 2020 Jan 2. Circ Res. 2020. PMID: 31895658 Free PMC article. Clinical Trial.
-
Effect of Vitamin D and ω-3 Fatty Acid Supplementation on Risk of Age-Related Macular Degeneration: An Ancillary Study of the VITAL Randomized Clinical Trial.JAMA Ophthalmol. 2020 Dec 1;138(12):1280-1289. doi: 10.1001/jamaophthalmol.2020.4409. JAMA Ophthalmol. 2020. PMID: 33119047 Free PMC article. Clinical Trial.
-
Marine omega-3 fatty acid supplementation and prevention of cardiovascular disease: update on the randomized trial evidence.Cardiovasc Res. 2023 Jun 13;119(6):1297-1309. doi: 10.1093/cvr/cvac172. Cardiovasc Res. 2023. PMID: 36378553 Free PMC article. Review.
-
Efficacy and Safety of Omega-3 Fatty Acids in the Prevention of Cardiovascular Disease: A Systematic Review and Meta-analysis.Cardiovasc Drugs Ther. 2024 Aug;38(4):799-817. doi: 10.1007/s10557-022-07379-z. Epub 2022 Sep 14. Cardiovasc Drugs Ther. 2024. PMID: 36103100 Review.
Cited by
-
Biomarkers of glucose-insulin homeostasis and incident type 2 diabetes and cardiovascular disease: results from the Vitamin D and Omega-3 trial.Cardiovasc Diabetol. 2024 Nov 2;23(1):393. doi: 10.1186/s12933-024-02470-1. Cardiovasc Diabetol. 2024. PMID: 39488682 Free PMC article. Clinical Trial.
-
Lifestyle and behavioral factors and mitochondrial DNA copy number in a diverse cohort of mid-life and older adults.PLoS One. 2020 Aug 12;15(8):e0237235. doi: 10.1371/journal.pone.0237235. eCollection 2020. PLoS One. 2020. PMID: 32785256 Free PMC article.
-
Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of the management of high-risk population.Stroke Vasc Neurol. 2020 Sep;5(3):270-278. doi: 10.1136/svn-2020-000385. Epub 2020 Aug 13. Stroke Vasc Neurol. 2020. PMID: 32792457 Free PMC article. Review.
-
The Role of Resolvins: EPA and DHA Derivatives Can Be Useful in the Prevention and Treatment of Ischemic Stroke.Int J Mol Sci. 2020 Oct 15;21(20):7628. doi: 10.3390/ijms21207628. Int J Mol Sci. 2020. PMID: 33076354 Free PMC article. Review.
-
Understanding the Role of Polyunsaturated Fatty Acids in the Development and Prevention of Cancer.Cancer Treat Res. 2024;191:57-93. doi: 10.1007/978-3-031-55622-7_3. Cancer Treat Res. 2024. PMID: 39133404 Review.
References
-
- Mozaffarian D, Wu JH. Omega-3 fatty acids and cardiovascular disease: effects on risk factors, molecular pathways, and clinical events. J Am Coll Cardiol. 2011;58:2047–67. - PubMed
-
- Rizos EC, Elisaf MS. Does supplementation with omega-3 PUFAs add to the prevention of cardiovascular disease? Curr Cardiol Rep. 2017;19:47. - PubMed
-
- Gerber M Omega-3 fatty acids and cancers: a systematic update review of epidemiological studies. Br J Nutr. 2012;107 Suppl 2:S228–39. - PubMed
-
- Manson JE, Bassuk SS, Lee IM, et al. The VITamin D and OmegA-3 TriaL (VITAL): Rationale and design of a large randomized controlled trial of vitamin D and marine omega-3 fatty acid supplements for the primary prevention of cancer and cardiovascular disease. Contemp Clin Trials. 2012;33:159–71. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources