

Dialysis Prescription and Sudden Death
- PMID: 30413252
- PMCID: PMC6392037
- DOI: 10.1016/j.semnephrol.2018.08.003
Dialysis Prescription and Sudden Death
Abstract
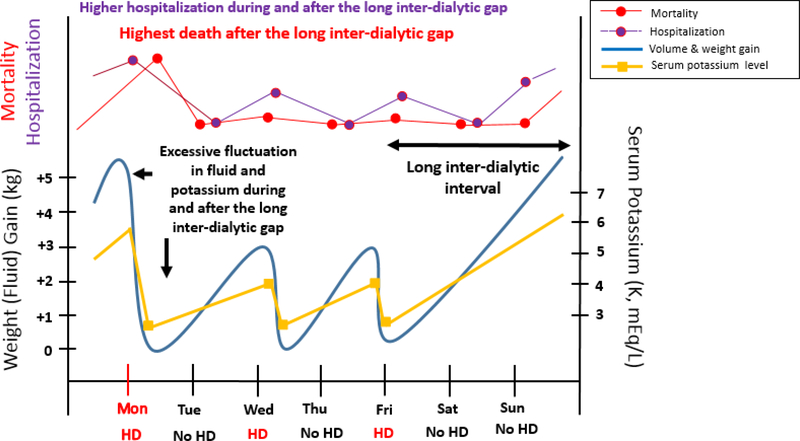
In the United States, end-stage renal disease patients receiving hemodialysis have an exceedingly high risk of sudden cardiac death (SCD), accounting for 29% of death events, likely relating to their uremic milieu, recurring exposure to fluid and electrolyte fluxes, and underlying cardiovascular pathology. Furthermore, epidemiologic studies have shown that SCD events, as well as mortality and hospitalizations, occur most frequently on the first dialysis day after the long interdialytic gap, suggesting that abrupt fluctuations in the accumulation and removal of electrolytes, fluid, and uremic toxins over the dialysis cycle may be contributory. Some population-based observational studies have suggested that lower dialysate potassium concentrations appear to be associated with a heightened risk of postdialysis cardiac arrest in hemodialysis patients, although the optimal serum-to-dialysate potassium gradient remains unclear. Some observational studies have suggested that low dialysate calcium concentrations and high serum-to-dialysate calcium gradients may predispose patients to SCD. There is ongoing controversy about an association between higher dialysate bicarbonate concentrations and higher risk of cardiac arrest, likely owing to confounding by indication. Some observational studies also have shown that large interdialytic weight gains, fluid retention, and high ultrafiltration rates are linked with higher risk of SCD and mortality. However, there remains considerable controversy regarding the pros and cons of designating a specific upper ultrafiltration limit with extended treatment times as a clinical practice measure, and further studies are needed to define the optimal tools, metrics, targets, and implementation measures for volume control in the hemodialysis population. In this review, we highlight the epidemiology and pathophysiology of how specific aspects of the hemodialysis procedure may relate to the risk of SCD, as well as preventative strategies and future research directions that can address this risk.
Keywords: Sudden cardiac death; electrolytes; hemodialysis; volume.
Copyright © 2018. Published by Elsevier Inc.
Conflict of interest statement
Conflicts of Interest:
None.
Figures
Similar articles
-
Dialysate and serum potassium in hemodialysis.Am J Kidney Dis. 2015 Jul;66(1):125-32. doi: 10.1053/j.ajkd.2015.02.322. Epub 2015 Mar 28. Am J Kidney Dis. 2015. PMID: 25828570 Review.
-
Sudden Cardiac Death Among Hemodialysis Patients.Am J Kidney Dis. 2017 May;69(5):684-695. doi: 10.1053/j.ajkd.2016.12.006. Epub 2017 Feb 17. Am J Kidney Dis. 2017. PMID: 28223004 Free PMC article. Review.
-
Dialysate Potassium, Serum Potassium, Mortality, and Arrhythmia Events in Hemodialysis: Results From the Dialysis Outcomes and Practice Patterns Study (DOPPS).Am J Kidney Dis. 2017 Feb;69(2):266-277. doi: 10.1053/j.ajkd.2016.09.015. Epub 2016 Nov 17. Am J Kidney Dis. 2017. PMID: 27866964 Free PMC article.
-
[Treatment of electrolyte disorders by hemodialysis].G Ital Nefrol. 2011 Jul-Aug;28(4):408-15. G Ital Nefrol. 2011. PMID: 21809310 Review. Italian.
-
Effect of Bicarbonate-Buffered Dialysate on Ventricular Arrhythmias in Hemodialysis Patients.Am J Nephrol. 2019;49(1):74-80. doi: 10.1159/000495846. Epub 2019 Jan 2. Am J Nephrol. 2019. PMID: 30602157
Cited by
-
Hemodialysis Procedure-Associated Autonomic Imbalance and Cardiac Arrhythmias: Insights From Continuous 14-Day ECG Monitoring.J Am Heart Assoc. 2019 Oct;8(19):e013748. doi: 10.1161/JAHA.119.013748. Epub 2019 Sep 28. J Am Heart Assoc. 2019. PMID: 31564195 Free PMC article.
-
Hidden risks associated with conventional short intermittent hemodialysis: A call for action to mitigate cardiovascular risk and morbidity.World J Nephrol. 2022 Mar 25;11(2):39-57. doi: 10.5527/wjn.v11.i2.39. World J Nephrol. 2022. PMID: 35433339 Free PMC article. Review.
-
A simple modification of dialysate potassium: its impact on plasma potassium concentrations and the electrocardiogram.Clin Kidney J. 2019 Nov 26;14(1):390-397. doi: 10.1093/ckj/sfz157. eCollection 2021 Jan. Clin Kidney J. 2019. PMID: 33564443 Free PMC article.
-
Epidemiological analysis of death among patients on maintenance hemodialysis: results from the beijing blood purification quality Control and Improvement Center.BMC Nephrol. 2023 Aug 15;24(1):236. doi: 10.1186/s12882-023-03271-6. BMC Nephrol. 2023. PMID: 37582779 Free PMC article.
-
Direct arterial puncture for hemodialysis, a neglected but simple and valuable vascular access.BMC Nephrol. 2022 Jun 23;23(1):221. doi: 10.1186/s12882-022-02836-1. BMC Nephrol. 2022. PMID: 35739470 Free PMC article.
References
-
- US Renal Data System. USRDS 2015 Annual Data Report: Atlas of End-Stage Renal Disease in the United States. Bethesda, MD; 2015.
-
- Cheung AK, Sarnak MJ, Yan G, et al. Cardiac diseases in maintenance hemodialysis patients: results of the HEMO Study. Kidney international. 2004;65(6):2380–2389. - PubMed
-
- Wanner C, Krane V, Marz W, et al. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. The New England journal of medicine. 2005;353(3):238–248. - PubMed
-
- Wheeler DC, London GM, Parfrey PS, et al. Effects of cinacalcet on atherosclerotic and nonatherosclerotic cardiovascular events in patients receiving hemodialysis: the EValuation Of Cinacalcet HCl Therapy to Lower CardioVascular Events (EVOLVE) trial. J Am Heart Assoc. 2014;3(6):e001363. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
