

Monocyte-to-Lymphocyte Ratio Is Associated With Tuberculosis Disease and Declines With Anti-TB Treatment in HIV-Infected Children
- PMID: 30399036
- PMCID: PMC6448767
- DOI: 10.1097/QAI.0000000000001893
Monocyte-to-Lymphocyte Ratio Is Associated With Tuberculosis Disease and Declines With Anti-TB Treatment in HIV-Infected Children
Abstract
Background: The blood monocyte-to-lymphocyte ratio (MLR) is associated with active tuberculosis (TB) in adults but has not been evaluated as a TB diagnostic biomarker in HIV-infected children in whom respiratory sampling is difficult.
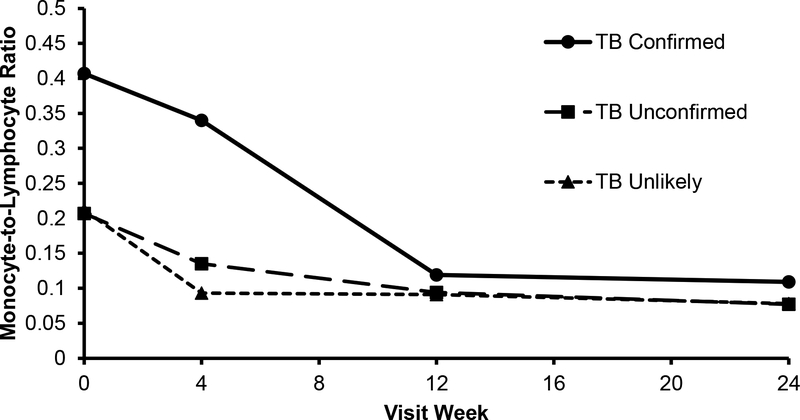
Setting: In a cohort of HIV-infected hospitalized Kenyan children initiating antiretroviral therapy, absolute monocyte and lymphocyte counts were determined at enrollment and 4, 12, and 24 weeks thereafter.
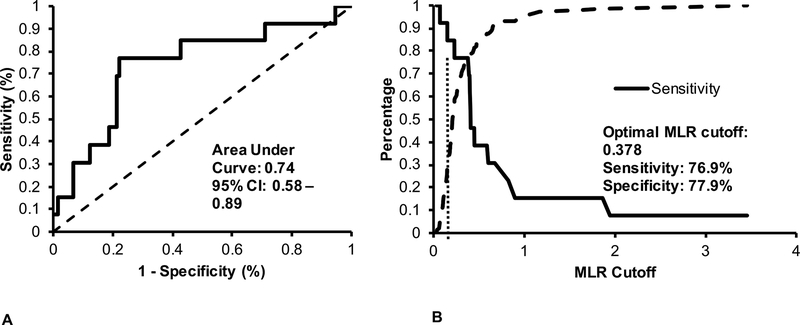
Methods: Children were classified as confirmed, unconfirmed, or unlikely pulmonary TB. Receiver operating characteristic curves of MLR cutoff values were generated to distinguish children with confirmed TB from those with unconfirmed and unlikely TB. General estimating equations were used to estimate change in the MLR over time by TB status.
Results: Of 160 children with median age 23 months, 13 (8.1%) had confirmed TB and 67 (41.9%) had unconfirmed TB. The median MLR among children with confirmed TB {0.407 [interquartile range (IQR) 0.378-0.675]} was higher than the MLR in children with unconfirmed [0.207 (IQR 0.148-0.348), P < 0.01] or unlikely [0.212 (IQR 0.138-0.391), P = 0.01] TB. The MLR above 0.378 identified children with confirmed TB with 77% sensitivity, 78% specificity, 24% positive predictive value, and 97% negative predictive value. After TB treatment, the median MLR declined in children with confirmed TB and levels were similar to children with unlikely TB after 12 weeks.
Conclusions: The blood MLR distinguished HIV-infected children with confirmed TB from those with unlikely TB and declined with TB treatment. The MLR may be a useful diagnostic tool for TB in settings where respiratory-based microbiologic confirmation is inaccessible.
Figures
Similar articles
-
Clinical correlate of tuberculosis in HIV co-infected children at the University of Abuja Teaching Hospital, Gwagwalada, Nigeria.Niger J Clin Pract. 2011 Apr-Jun;14(2):206-11. doi: 10.4103/1119-3077.84018. Niger J Clin Pract. 2011. PMID: 21860141
-
Characteristics of HIV-infected tuberculosis patients in Thailand.Southeast Asian J Trop Med Public Health. 2009 Jan;40(1):93-103. Southeast Asian J Trop Med Public Health. 2009. PMID: 19323040
-
British HIV Association guidelines for the treatment of TB/HIV coinfection 2011.HIV Med. 2011 Oct;12(9):517-24. doi: 10.1111/j.1468-1293.2011.00954.x. HIV Med. 2011. PMID: 21951595 No abstract available.
-
Optimal Timing of Antiretroviral Therapy Initiation for HIV-Infected Adults With Newly Diagnosed Pulmonary Tuberculosis: A Systematic Review and Meta-analysis.Ann Intern Med. 2015 Jul 7;163(1):32-9. doi: 10.7326/M14-2979. Ann Intern Med. 2015. PMID: 26148280 Review.
-
Impact of tuberculosis preventive therapy on tuberculosis and mortality in HIV-infected children.Cochrane Database Syst Rev. 2009 Jan 21;(1):CD006418. doi: 10.1002/14651858.CD006418.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2017 Aug 29;8:CD006418. doi: 10.1002/14651858.CD006418.pub3. PMID: 19160285 Updated. Review.
Cited by
-
HIV-Associated Tuberculosis in Children and Adolescents: Evolving Epidemiology, Screening, Prevention and Management Strategies.Pathogens. 2021 Dec 29;11(1):33. doi: 10.3390/pathogens11010033. Pathogens. 2021. PMID: 35055981 Free PMC article. Review.
-
Single-cell profiling reveals distinct subsets of CD14+ monocytes drive blood immune signatures of active tuberculosis.Front Immunol. 2023 Jan 11;13:1087010. doi: 10.3389/fimmu.2022.1087010. eCollection 2022. Front Immunol. 2023. PMID: 36713384 Free PMC article.
-
Circulating mitochondrial cell-free DNA dynamics in patients with mycobacterial pulmonary infections: Potential for a novel biomarker of disease.Front Immunol. 2022 Nov 15;13:1040947. doi: 10.3389/fimmu.2022.1040947. eCollection 2022. Front Immunol. 2022. PMID: 36466831 Free PMC article.
-
Association of Single Nucleotide Polymorphism rs17580 with Smoking and Pulmonary Tuberculosis.J Healthc Eng. 2022 Apr 9;2022:6984403. doi: 10.1155/2022/6984403. eCollection 2022. J Healthc Eng. 2022. Retraction in: J Healthc Eng. 2023 Jul 12;2023:9837380. doi: 10.1155/2023/9837380. PMID: 35437467 Free PMC article. Retracted.
-
Monocyte to lymphocyte ratio and hemoglobin level to predict tuberculosis after antiretroviral therapy initiation.AIDS. 2024 Jan 1;38(1):31-38. doi: 10.1097/QAD.0000000000003713. Epub 2023 Sep 8. AIDS. 2024. PMID: 37696248 Free PMC article.
References
-
- Cox JA, Lukande RL, Lucas S, Nelson AM, Van Marck E, Colebunders R. Autopsy causes of death in HIV-positive individuals in sub-Saharan Africa and correlation with clinical diagnoses. AIDS Rev. 2010;12(4):183–194. - PubMed
-
- World Health Organization. Global tuberculosis report 2017. November 30, 2017. Available at: http://www.who.int/tb/publications/global_report/en/0.
-
- Perez-Velez CM, Roya-Pabon CL, Marais BJ. A systematic approach to diagnosing intra-thoracic tuberculosis in children. J Infect. 2017;74 Suppl 1:S74–S83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
