

A patient-level pooled analysis of treatment-shortening regimens for drug-susceptible pulmonary tuberculosis
- PMID: 30397355
- PMCID: PMC6685538
- DOI: 10.1038/s41591-018-0224-2
A patient-level pooled analysis of treatment-shortening regimens for drug-susceptible pulmonary tuberculosis
Erratum in
-
Publisher Correction: A patient-level pooled analysis of treatment-shortening regimens for drug-susceptible pulmonary tuberculosis.Nat Med. 2019 Jan;25(1):190. doi: 10.1038/s41591-018-0294-1. Nat Med. 2019. PMID: 30429542 Free PMC article.
Abstract
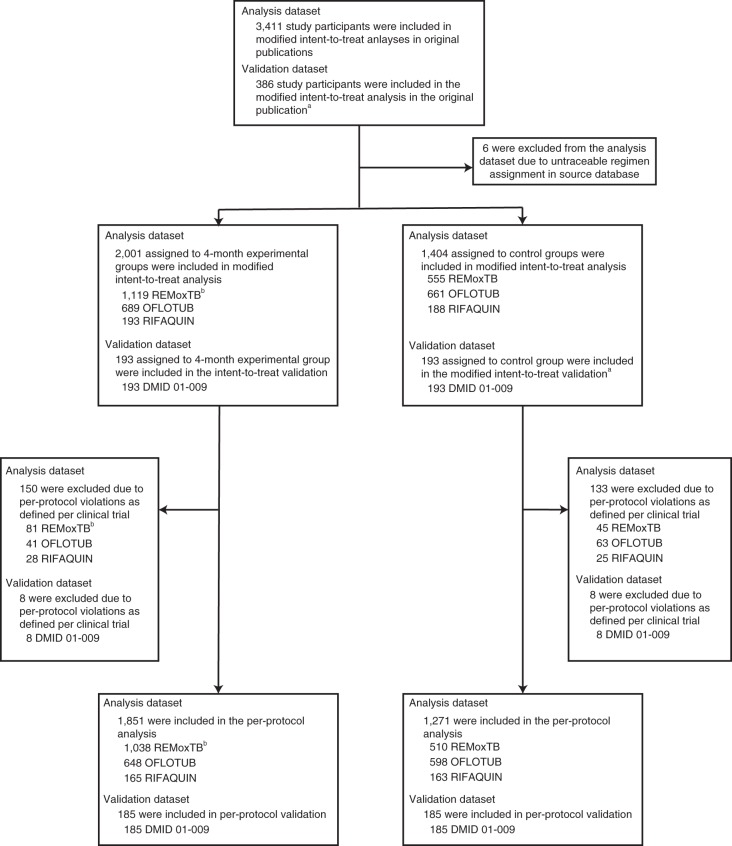
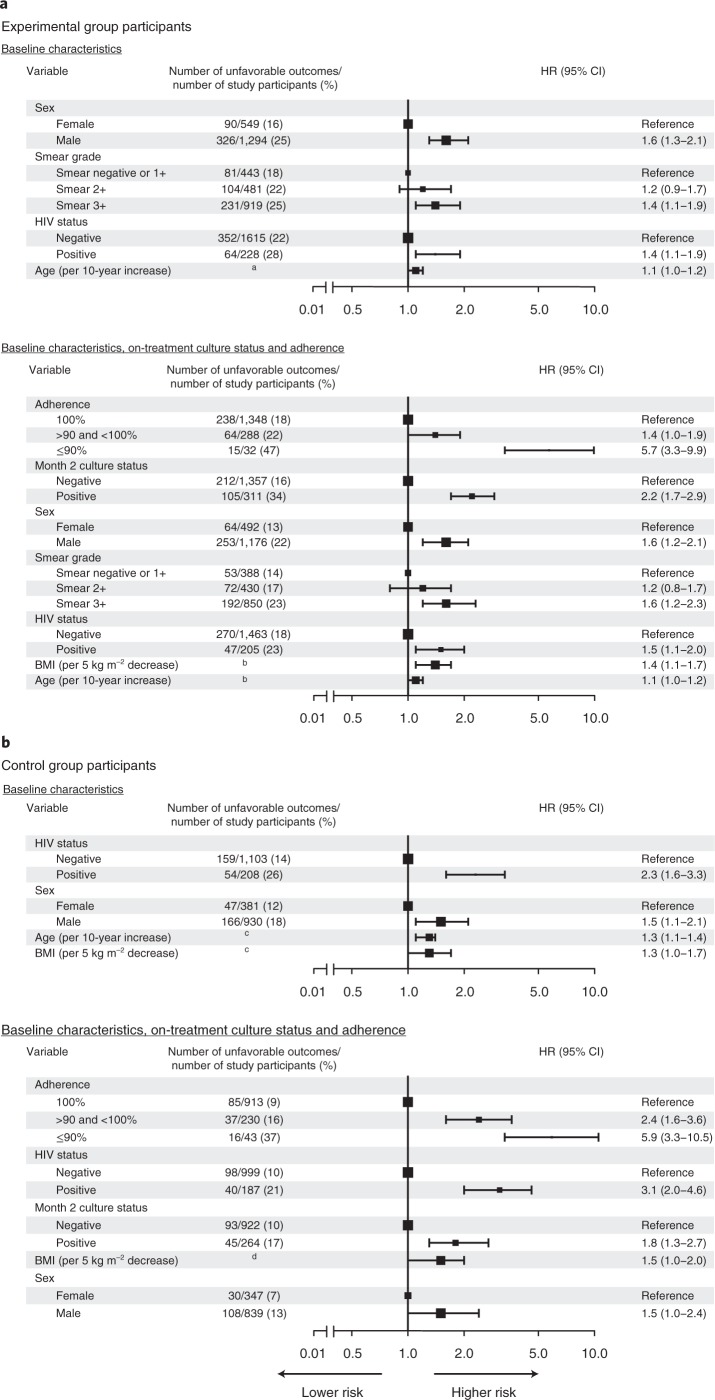
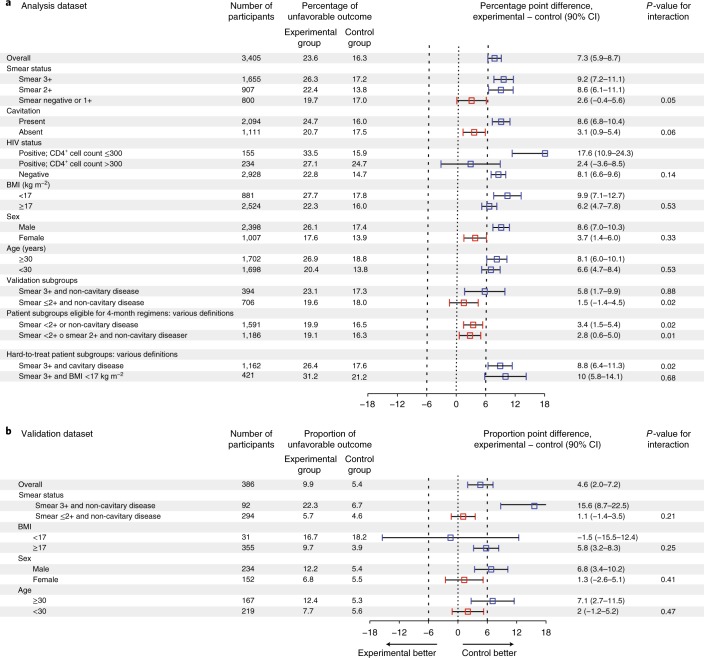
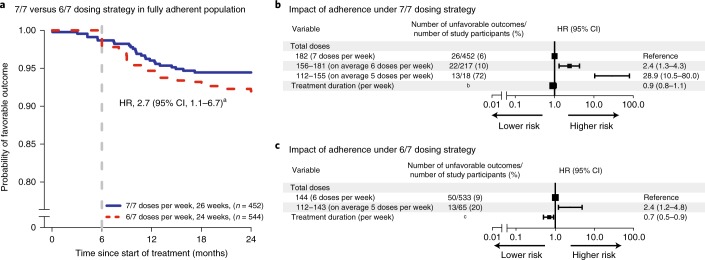
Tuberculosis kills more people than any other infectious disease. Three pivotal trials testing 4-month regimens failed to meet non-inferiority margins; however, approximately four-fifths of participants were cured. Through a pooled analysis of patient-level data with external validation, we identify populations eligible for 4-month treatment, define phenotypes that are hard to treat and evaluate the impact of adherence and dosing strategy on outcomes. In 3,405 participants included in analyses, baseline smear grade of 3+ relative to <2+, HIV seropositivity and adherence of ≤90% were significant risk factors for unfavorable outcome. Four-month regimens were non-inferior in participants with minimal disease defined by <2+ sputum smear grade or non-cavitary disease. A hard-to-treat phenotype, defined by high smear grades and cavitation, may require durations >6 months to cure all. Regimen duration can be selected in order to improve outcomes, providing a stratified medicine approach as an alternative to the 'one-size-fits-all' treatment currently used worldwide.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
A stratified approach to tuberculosis treatment.Nat Med. 2018 Nov;24(11):1639-1641. doi: 10.1038/s41591-018-0244-y. Nat Med. 2018. PMID: 30401868 No abstract available.
Similar articles
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Lamotrigine versus levetiracetam or zonisamide for focal epilepsy and valproate versus levetiracetam for generalised and unclassified epilepsy: two SANAD II non-inferiority RCTs.Health Technol Assess. 2021 Dec;25(75):1-134. doi: 10.3310/hta25750. Health Technol Assess. 2021. PMID: 34931602 Clinical Trial.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Undernutrition as a risk factor for tuberculosis disease.Cochrane Database Syst Rev. 2024 Jun 11;6(6):CD015890. doi: 10.1002/14651858.CD015890.pub2. Cochrane Database Syst Rev. 2024. PMID: 38860538 Free PMC article. Review.
-
Depressing time: Waiting, melancholia, and the psychoanalytic practice of care.In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. PMID: 36137063 Free Books & Documents. Review.
Cited by
-
A leap forward in assessing host-directed therapies for tuberculosis.Lancet Respir Med. 2021 Aug;9(8):809-810. doi: 10.1016/S2213-2600(20)30528-2. Epub 2021 Mar 16. Lancet Respir Med. 2021. PMID: 33740467 Free PMC article. No abstract available.
-
Disease extent and anti-tubercular treatment response correlates with Mycobacterium tuberculosis-specific CD4 T-cell phenotype regardless of HIV-1 status.Clin Transl Immunology. 2020 Sep 28;9(9):e1176. doi: 10.1002/cti2.1176. eCollection 2020. Clin Transl Immunology. 2020. PMID: 33005414 Free PMC article.
-
Wirelessly observed therapy compared to directly observed therapy to confirm and support tuberculosis treatment adherence: A randomized controlled trial.PLoS Med. 2019 Oct 4;16(10):e1002891. doi: 10.1371/journal.pmed.1002891. eCollection 2019 Oct. PLoS Med. 2019. PMID: 31584944 Free PMC article. Clinical Trial.
-
Association of Single Nucleotide Polymorphism rs17580 with Smoking and Pulmonary Tuberculosis.J Healthc Eng. 2022 Apr 9;2022:6984403. doi: 10.1155/2022/6984403. eCollection 2022. J Healthc Eng. 2022. Retraction in: J Healthc Eng. 2023 Jul 12;2023:9837380. doi: 10.1155/2023/9837380. PMID: 35437467 Free PMC article. Retracted.
-
Predictors of slow clinical response and extended treatment in patients with extra-pulmonary tuberculosis in Pakistan, A hospital-based prospective study.PLoS One. 2021 Nov 12;16(11):e0259801. doi: 10.1371/journal.pone.0259801. eCollection 2021. PLoS One. 2021. PMID: 34767601 Free PMC article.
References
-
- World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care, 2017 Update (World Health Organization, Geneva, 2017).
