

Current appraisal of single inhaler triple therapy in COPD
- PMID: 30319248
- PMCID: PMC6167973
- DOI: 10.2147/COPD.S177333
Current appraisal of single inhaler triple therapy in COPD
Abstract
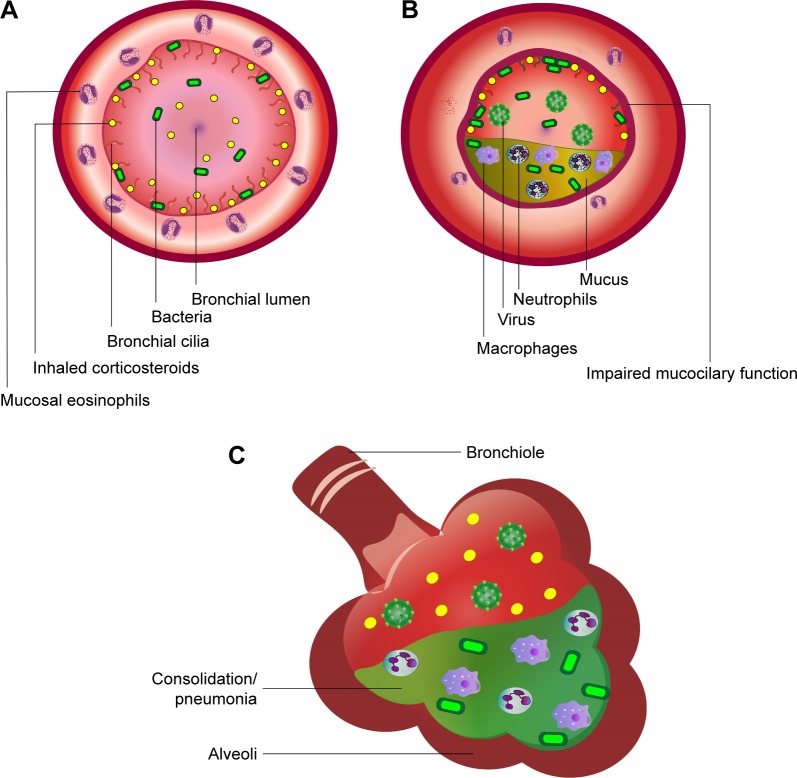
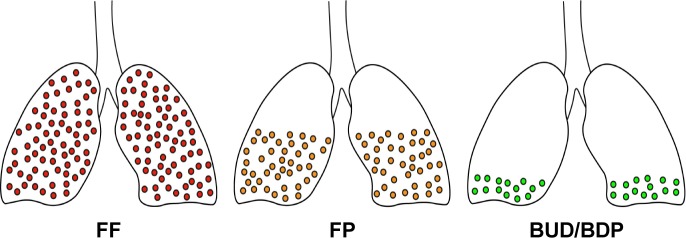
A single inhaler containing inhaled corticosteroid (ICS)/long-acting beta-agonist (LABA)/long-acting muscarinic antagonist (LAMA) is a more convenient way of delivering triple therapy in patients with COPD. Single triple therapy has been shown to be superior at reducing exacerbations and improving quality of life compared to LABA/LAMA, especially in patients with a prior history of frequent exacerbations and blood eosinophilia, who have ICS responsive disease. The corollary is that patients with infrequent exacerbations who are noneosinophilic may be safely de-escalated from triple therapy to LABA/LAMA without loss of control. Pointedly, there is a substantially increased risk of pneumonia associated with the triple therapy containing fluticasone furoate but not beclometasone dipropionate or budesonide. Since triple therapy is also better than ICS/LABA at reducing exacerbations and improving lung function, symptoms, and quality of life, this brings into question the rationale for using ICS/LABA. Hence, we propose a simplified pragmatic decision process based on symptoms, prior to exacerbation history, and blood eosinophils to select which patients should be given a single triple inhaler or LABA/LAMA. Differences in patient preference of inhaler device, formulations and drugs will also determine which triple inhaler prescribers elect to use.
Keywords: COPD; exacerbation; inhaled corticosteroid; long-acting beta-agonist; long-acting muscarinic antagonist; lung function.
Conflict of interest statement
Disclosure Dr Lipworth reports grants and personal fees from AZ, personal fees and other from Teva, personal fees from Novartis, nonfinancial support from GSK, grants and personal fees from Chiesi, grants and personal fees from Boerhinger, during the conduct of the study; grants and personal fees from Meda/Mylan, grants from Janssen, grants from Roche, personal fees from Lupin, grants and personal fees from Boerhinger Ingelheim, grants and personal fees from Chiesi, personal fees from Cipla, personal fees from Sandoz, personal fees from Dr Reddys, grants and personal fees from Sanofi, personal fees from Circassia, outside the submitted work. Dr Kuo reports personal fees and nonfinancial support from Pfizer, outside the submitted work. Dr Jabbal reports personal fees and nonfinancial support from Chiesi Pharma, personal fees and nonfinancial support from Pfizer, nonfinancial support and other from Napp, personal fees and nonfinancial support from AstraZeneca, nonfinancial support from Teva, personal fees and nonfinancial support from Mylan, personal fees from Boehringer Ingelheim, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
The effects of single inhaler triple therapy vs single inhaler dual therapy or separate triple therapy for the management of chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized controlled trials.Int J Chron Obstruct Pulmon Dis. 2019 Jul 11;14:1539-1548. doi: 10.2147/COPD.S200846. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 31371939 Free PMC article.
-
Efficacy of Budesonide/Glycopyrronium/Formoterol Fumarate Metered Dose Inhaler (BGF MDI) Versus Other Inhaled Corticosteroid/Long-Acting Muscarinic Antagonist/Long-Acting β2-Agonist (ICS/LAMA/LABA) Triple Combinations in COPD: A Systematic Literature Review and Network Meta-analysis.Adv Ther. 2020 Jun;37(6):2956-2975. doi: 10.1007/s12325-020-01311-3. Epub 2020 Apr 25. Adv Ther. 2020. PMID: 32335859 Free PMC article.
-
Triple therapy (ICS/LABA/LAMA) in COPD: time for a reappraisal.Int J Chron Obstruct Pulmon Dis. 2018 Dec 12;13:3971-3981. doi: 10.2147/COPD.S185975. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 30587953 Free PMC article. Review.
-
Role of Long-Acting Muscarinic Antagonist/Long-Acting β2-Agonist Therapy in Chronic Obstructive Pulmonary Disease.Ann Pharmacother. 2017 Aug;51(8):696-705. doi: 10.1177/1060028017705149. Epub 2017 Apr 14. Ann Pharmacother. 2017. PMID: 28410560 Review.
-
Single-inhaler triple therapy in patients with chronic obstructive pulmonary disease: a systematic review.Respir Res. 2019 Nov 4;20(1):242. doi: 10.1186/s12931-019-1213-9. Respir Res. 2019. PMID: 31684965 Free PMC article.
Cited by
-
The Impact of 52-Week Single Inhaler Device Triple Therapy versus Dual Therapy on the Mortality of COPD Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Life (Basel). 2022 Jan 25;12(2):173. doi: 10.3390/life12020173. Life (Basel). 2022. PMID: 35207460 Free PMC article. Review.
-
Weathering the Cytokine Storm in Susceptible Patients with Severe SARS-CoV-2 Infection.J Allergy Clin Immunol Pract. 2020 Jun;8(6):1798-1801. doi: 10.1016/j.jaip.2020.04.014. Epub 2020 Apr 18. J Allergy Clin Immunol Pract. 2020. PMID: 32311489 Free PMC article. No abstract available.
-
Long-Term Safety and Efficacy of Budesonide/Glycopyrrolate/Formoterol Fumarate Metered Dose Inhaler Formulated Using Co-Suspension Delivery Technology in Japanese Patients with COPD.Int J Chron Obstruct Pulmon Dis. 2019 Dec 23;14:2993-3002. doi: 10.2147/COPD.S220861. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 31920296 Free PMC article. Clinical Trial.
-
Withdrawal of inhaled corticosteroids in COPD patients: rationale and algorithms.Int J Chron Obstruct Pulmon Dis. 2019 Jun 10;14:1267-1280. doi: 10.2147/COPD.S207775. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 31354256 Free PMC article. Review.
-
Risk of Pneumonia in Patients with COPD Initiating Fixed Dose Inhaled Corticosteroid (ICS) / Long-Acting Bronchodilator (LABD) Formulations Containing Extrafine Beclometasone Dipropionate versus Patients Initiating LABD Without ICS.Pragmat Obs Res. 2024 Jan 20;15:1-16. doi: 10.2147/POR.S438031. eCollection 2024. Pragmat Obs Res. 2024. PMID: 38274639 Free PMC article.
References
-
- Lipworth B, Jabbal S. A pragmatic approach to simplify inhaler therapy for COPD. Lancet Respir Med. 2017;5(9):679–681. - PubMed
-
- Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. - PubMed
-
- Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. - PubMed
-
- Kistemaker LE, Oenema TA, Meurs H, Gosens R. Regulation of airway inflammation and remodeling by muscarinic receptors: perspectives on anticholinergic therapy in asthma and COPD. Life Sci. 2012;91(21–22):1126–1133. - PubMed
-
- Suissa S. Number needed to treat in COPD: exacerbations versus pneumonias. Thorax. 2013;68(6):540–543. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
