

The 10th Biennial Hatter Cardiovascular Institute workshop: cellular protection-evaluating new directions in the setting of myocardial infarction, ischaemic stroke, and cardio-oncology
- PMID: 30310998
- PMCID: PMC6182684
- DOI: 10.1007/s00395-018-0704-z
The 10th Biennial Hatter Cardiovascular Institute workshop: cellular protection-evaluating new directions in the setting of myocardial infarction, ischaemic stroke, and cardio-oncology
Abstract
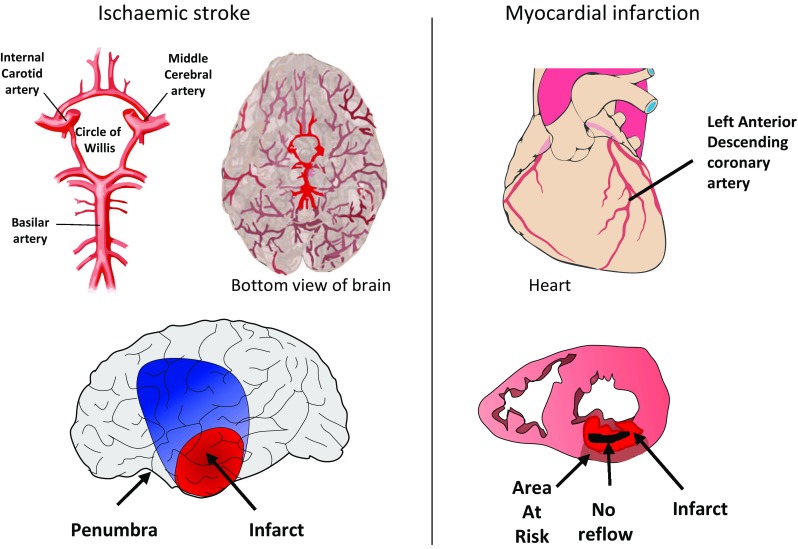
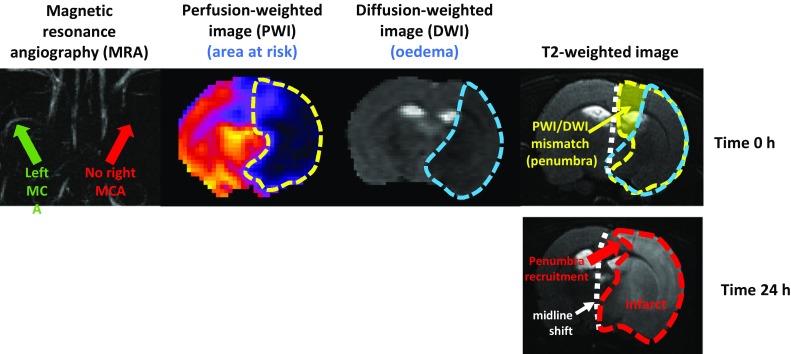
Due to its poor capacity for regeneration, the heart is particularly sensitive to the loss of contractile cardiomyocytes. The onslaught of damage caused by ischaemia and reperfusion, occurring during an acute myocardial infarction and the subsequent reperfusion therapy, can wipe out upwards of a billion cardiomyocytes. A similar program of cell death can cause the irreversible loss of neurons in ischaemic stroke. Similar pathways of lethal cell injury can contribute to other pathologies such as left ventricular dysfunction and heart failure caused by cancer therapy. Consequently, strategies designed to protect the heart from lethal cell injury have the potential to be applicable across all three pathologies. The investigators meeting at the 10th Hatter Cardiovascular Institute workshop examined the parallels between ST-segment elevation myocardial infarction (STEMI), ischaemic stroke, and other pathologies that cause the loss of cardiomyocytes including cancer therapeutic cardiotoxicity. They examined the prospects for protection by remote ischaemic conditioning (RIC) in each scenario, and evaluated impasses and novel opportunities for cellular protection, with the future landscape for RIC in the clinical setting to be determined by the outcome of the large ERIC-PPCI/CONDI2 study. It was agreed that the way forward must include measures to improve experimental methodologies, such that they better reflect the clinical scenario and to judiciously select combinations of therapies targeting specific pathways of cellular death and injury.
Keywords: Anthracycline cardiotoxicity; Cardioprotection; Ischaemic stroke; Myocardial ischaemia; Neuroprotection; Reperfusion.
Conflict of interest statement
Dr Richard Carr is an employee of MSD A/S, Copenhagen V, Denmark. There are no other conflicts of interest to declare.
Figures
Similar articles
-
Remote ischaemic conditioning: defining critical criteria for success-report from the 11th Hatter Cardiovascular Workshop.Basic Res Cardiol. 2022 Aug 15;117(1):39. doi: 10.1007/s00395-022-00947-2. Basic Res Cardiol. 2022. PMID: 35970954 Free PMC article. Review.
-
Novel targets and future strategies for acute cardioprotection: Position Paper of the European Society of Cardiology Working Group on Cellular Biology of the Heart.Cardiovasc Res. 2017 May 1;113(6):564-585. doi: 10.1093/cvr/cvx049. Cardiovasc Res. 2017. PMID: 28453734 Review.
-
Cardioprotection by combined intrahospital remote ischaemic perconditioning and postconditioning in ST-elevation myocardial infarction: the randomized LIPSIA CONDITIONING trial.Eur Heart J. 2015 Nov 21;36(44):3049-57. doi: 10.1093/eurheartj/ehv463. Epub 2015 Sep 17. Eur Heart J. 2015. PMID: 26385956 Clinical Trial.
-
Effect of remote ischaemic conditioning on clinical outcomes in patients with acute myocardial infarction (CONDI-2/ERIC-PPCI): a single-blind randomised controlled trial.Lancet. 2019 Oct 19;394(10207):1415-1424. doi: 10.1016/S0140-6736(19)32039-2. Epub 2019 Sep 6. Lancet. 2019. PMID: 31500849 Free PMC article. Clinical Trial.
-
Preconditioning and postconditioning: underlying mechanisms and clinical application.Atherosclerosis. 2009 Jun;204(2):334-41. doi: 10.1016/j.atherosclerosis.2008.10.029. Epub 2008 Nov 5. Atherosclerosis. 2009. PMID: 19081095 Review.
Cited by
-
Intracoronary Administration of Microencapsulated HGF in a Reperfused Myocardial Infarction Swine Model.J Cardiovasc Dev Dis. 2023 Feb 17;10(2):86. doi: 10.3390/jcdd10020086. J Cardiovasc Dev Dis. 2023. PMID: 36826582 Free PMC article.
-
SERCA Overexpression Improves Mitochondrial Quality Control and Attenuates Cardiac Microvascular Ischemia-Reperfusion Injury.Mol Ther Nucleic Acids. 2020 Sep 16;22:696-707. doi: 10.1016/j.omtn.2020.09.013. eCollection 2020 Dec 4. Mol Ther Nucleic Acids. 2020. PMID: 33230467 Free PMC article.
-
Inhibition of cardiomyocyte Sprouty1 protects from cardiac ischemia-reperfusion injury.Basic Res Cardiol. 2019 Jan 11;114(2):7. doi: 10.1007/s00395-018-0713-y. Basic Res Cardiol. 2019. PMID: 30635790 Free PMC article.
-
The Role of Extracellular DNA and Histones in Ischaemia-Reperfusion Injury of the Myocardium.Cardiovasc Drugs Ther. 2020 Feb;34(1):123-131. doi: 10.1007/s10557-020-06946-6. Cardiovasc Drugs Ther. 2020. PMID: 32062794 Free PMC article. Review.
-
Mitochondrial and mitochondrial-independent pathways of myocardial cell death during ischaemia and reperfusion injury.J Cell Mol Med. 2020 Apr;24(7):3795-3806. doi: 10.1111/jcmm.15127. Epub 2020 Mar 10. J Cell Mol Med. 2020. PMID: 32155321 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
