

Comparison of pre-treatment with OCPs or estradiol valerate vs. no pre-treatment prior to GnRH antagonist used for IVF cycles: An RCT
- PMID: 30288488
- PMCID: PMC6163045
Comparison of pre-treatment with OCPs or estradiol valerate vs. no pre-treatment prior to GnRH antagonist used for IVF cycles: An RCT
Abstract
Background: Both oral contraceptive pills (OCPs) and estradiol valerate (E2) have been used to schedule a gonadotropin-releasing hormone antagonist in vitro fertilization (IVF) cycles. Since the suppression of follicle-stimulating hormone by OCPs can stay 5-7 days after stopping the pills, it seems that starting the gonadotropin-releasing hormone (GnRH) after 6 days of pre-treatment discontinuation may be important in IVF outcomes.
Objective: The aim of the present study was to determine the number of mature oocyte and pregnancy rate of three pretreatment methods for fresh embryo transfer cycles.
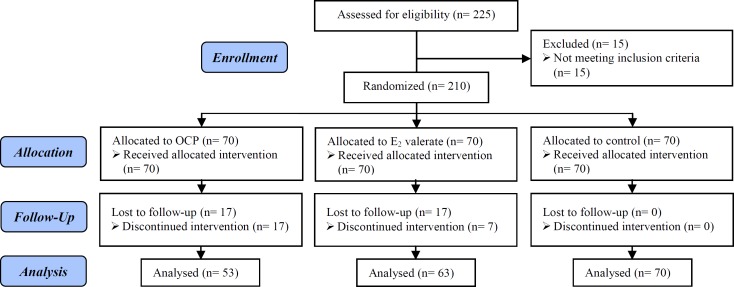
Materials and methods: In this randomized controlled trial, two-hundred ten women (18-35 yr and less than 2 previous IVF attempts) undergoing IVF with the GnRH antagonist protocol were randomized to the OCP, E2, and no pretreatment arms. OCP group (n=53) received OCP (ethinyl estradiol30 μg and levonorgestrel150 μg), E2 group (n=63) received 4 mg/day oral E2 (17β-E2) for 10 days from day 20 of the previous cycle and GnRH antagonist stimulation was started 6 days after the interruption of OCP and E2. The control group (n =70) did not receive any pretreatment.
Results: No significant difference was observed in the mean number of the mature oocyte, endometrial thickness, and embryo quality. The pregnancy rate in E2 group was higher than the two other groups (42.9% vs 39.6% and 34.3% in OCP and control group, respectively), but the difference was not statistically significant (p=0.59).
Conclusion: It seems OCP or E2 pretreatment could not improve the fresh IVF-embryo transfer outcomes.
Keywords: Estradiol; GnRH antagonist; IVF; Oral contraceptives.
Conflict of interest statement
It should be noted that there was no association between the authors and any organization or institution. The authors have no competing interests or other interests that might be perceived to influence the results and discussion reported in this paper.
Similar articles
-
Cycle scheduling for in vitro fertilization with oral contraceptive pills versus oral estradiol valerate: a randomized, controlled trial.Reprod Biol Endocrinol. 2013 Sep 28;11:96. doi: 10.1186/1477-7827-11-96. Reprod Biol Endocrinol. 2013. PMID: 24074027 Free PMC article. Clinical Trial.
-
Use of steroid pre-treatments in IVF-ICSI cycles with GnRH antagonist protocol and their impact on gestational outcomes.J Obstet Gynaecol. 2022 Apr;42(3):478-484. doi: 10.1080/01443615.2021.1916806. Epub 2021 Jun 21. J Obstet Gynaecol. 2022. PMID: 34151671 Clinical Trial.
-
Pretreatment with oral contraceptive pills to identify poor responders that may benefit from rLH supplementation during GnRH-antagonist treatment for IVF: A pilot perspective study proposal.Exp Ther Med. 2015 Nov;10(5):1692-1696. doi: 10.3892/etm.2015.2734. Epub 2015 Sep 8. Exp Ther Med. 2015. PMID: 26640538 Free PMC article.
-
Steroids pretreatment in assisted reproduction cycles.J Steroid Biochem Mol Biol. 2014 Jan;139:114-21. doi: 10.1016/j.jsbmb.2013.04.007. Epub 2013 May 16. J Steroid Biochem Mol Biol. 2014. PMID: 23685395 Review.
-
Gonadotropin-releasing hormone agonist versus HCG for oocyte triggering in antagonist assisted reproductive technology cycles.Cochrane Database Syst Rev. 2011 Jan 19;(1):CD008046. doi: 10.1002/14651858.CD008046.pub3. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2014 Oct 31;(10):CD008046. doi: 10.1002/14651858.CD008046.pub4 PMID: 21249699 Updated. Review.
Cited by
-
What is the optimal GnRH antagonist protocol for ovarian stimulation during ART treatment? A systematic review and network meta-analysis.Hum Reprod Update. 2023 May 2;29(3):307-326. doi: 10.1093/humupd/dmac040. Hum Reprod Update. 2023. PMID: 36594696 Free PMC article.
-
Estradiol pretreatment in GnRH antagonist protocol for IVF/ICSI treatment.Open Med (Wars). 2022 Nov 21;17(1):1811-1820. doi: 10.1515/med-2022-0594. eCollection 2022. Open Med (Wars). 2022. PMID: 36457798 Free PMC article.
-
Ovarian Stimulation in Assisted Reproductive Technology Cycles for Varied Patient Profiles: An Indian Perspective.J Hum Reprod Sci. 2022 Apr-Jun;15(2):112-125. doi: 10.4103/jhrs.jhrs_59_22. Epub 2022 Jun 30. J Hum Reprod Sci. 2022. PMID: 35928474 Free PMC article. Review.
References
-
- Frydman R, Forman R, Rainhorn JD, Belaisch-Allart J, Hazout A, Testart J. A new approach to follicular stimulation for in vitro fertilization: programmed oocyte retrieval. Fertil Steril. 1986;46:657–662. - PubMed
-
- Wardle PG, Foster PA, Mitchell JD, McLaughlin EA, Williams JA, Corrigan E, et al. Norethisterone treatment to control timing of IVF cycle. Hum Reprod. 1986;1:455–457. - PubMed
-
- Zorn JR, Boyer P, Guichard A. Never on a Sunday: programming for IVF-ET and GIFT. Lancet. 1987;1:385–386. - PubMed
-
- Gerli S, Remohí J, Partrizio P, Borrero C, Balmaceda JP, Silber SJ, et al. Programming of ovarian stimulation with norethindrone acetate in IVF/GIFT cycles. Hum Reprod. 1989;4:746–748. - PubMed
-
- Griesinger G, Venetis CA, Marx T, Diedrich K, Tarlatzis BC, Kolibianakis ME. Oral contraceptive pill pretreatment in ovarian stimulation with GnRH antagonists for IVF: a systematic review and meta-analyses. Fert Steril. 2008;90:1055–1063. - PubMed
LinkOut - more resources
Full Text Sources