

The biology and treatment of Merkel cell carcinoma: current understanding and research priorities
- PMID: 30287935
- PMCID: PMC6319370
- DOI: 10.1038/s41571-018-0103-2
The biology and treatment of Merkel cell carcinoma: current understanding and research priorities
Abstract
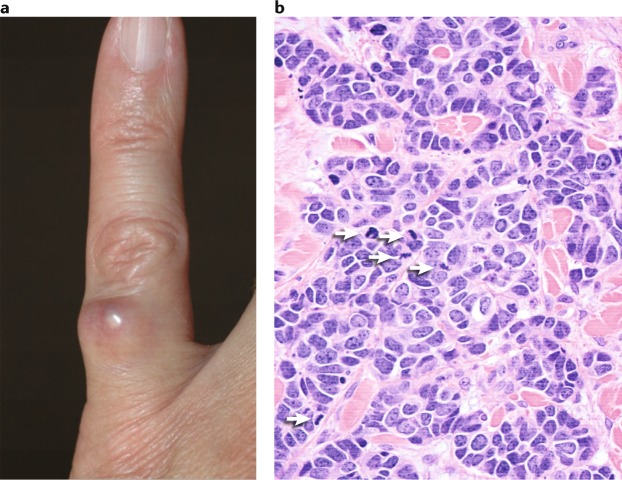
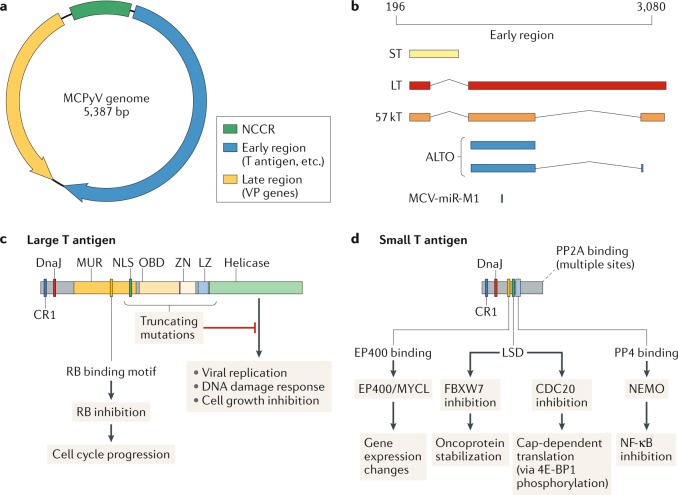
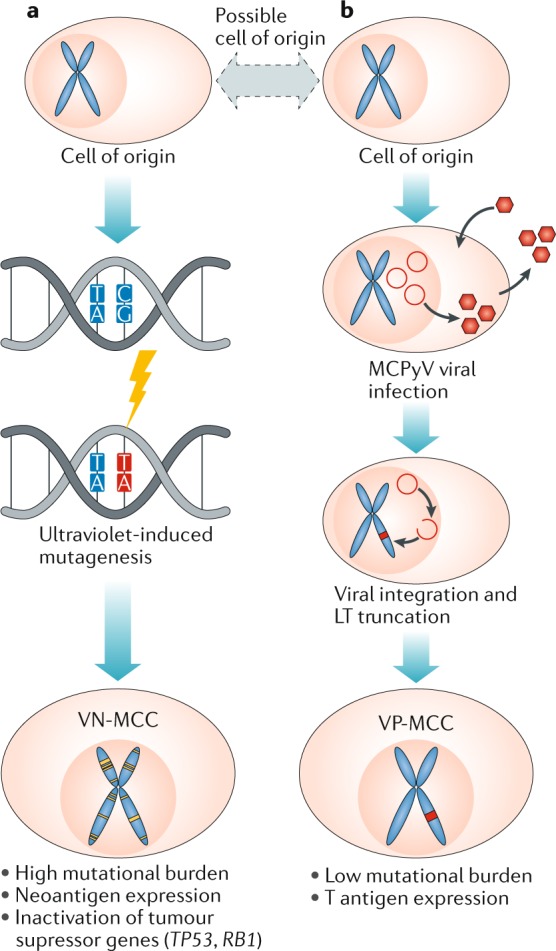
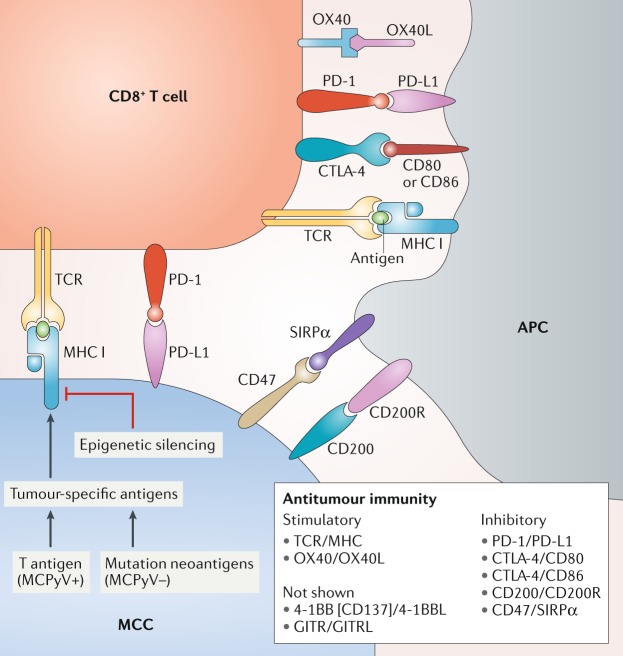
Merkel cell carcinoma (MCC) is a rare and aggressive skin cancer associated with advanced age and immunosuppression. Over the past decade, an association has been discovered between MCC and either integration of the Merkel cell polyomavirus, which likely drives tumorigenesis, or somatic mutations owing to ultraviolet-induced DNA damage. Both virus-positive and virus-negative MCCs are immunogenic, and inhibition of the programmed cell death protein 1 (PD-1)-programmed cell death 1 ligand 1 (PD-L1) immune checkpoint has proved to be highly effective in treating patients with metastatic MCC; however, not all patients have a durable response to immunotherapy. Despite these rapid advances in the understanding and management of patients with MCC, many basic, translational and clinical research questions remain unanswered. In March 2018, an International Workshop on Merkel Cell Carcinoma Research was held at the US National Cancer Institute, at which academic, government and industry experts met to identify the highest-priority research questions. Here, we review the biology and treatment of MCC and report the consensus-based recommendations agreed upon during the workshop.
Conflict of interest statement
The International Workshop for Merkel Cell Carcinoma Research, which included activities related to the preparation of this Consensus Statement, was supported by funding from Bristol-Myers Squibb (BMS), EMD Serono, the US National Cancer Institute and the US National Institute of Arthritis and Musculoskeletal and Skin Diseases. J.C.B. has received honoraria from Amgen, Merck Serono and Pfizer; he has received advisory board honoraria from Amgen, CureVac, eTheRNA, Lytix, Merck Serono, Novartis, Rigontec and Takeda; and he has received research funding from Boehringer Ingelheim, BMS and Merck Serono. S.B. reports research funding to his institution (the University of Washington, WA, USA) from Merck, BMS, EMD Serono, ImmuneDesign, NantKwest and Oncosec. S.B. has received honoraria for participation in advisory boards from EMD Serono and Genentech. S.P.D. has received consulting and travel support from EMD Serono. J.K. and M.H. are full-time employees of EMD Serono. M.M. is a full-time employee of Foundation Medicine. P.N. is a consultant of EMD Serono and Merck and reports research funding to his institution (the University of Washington, WA, USA) from BMS and EMD Serono. G.R. is an advisory board member and/or consultant of EMD Serono and Pfizer and owns stocks in Regeneron and Syros Pharmaceuticals. M.R. has served on the advisory boards of Merck and Novartis. M.T.T. serves on the advisory boards of Novartis, Myriad Genetics and Seattle Genetics. R.T. has received honoraria from Merck Serono. D.M.T. is a full-time employee of MedImmune. M.K.K.W. serves on the advisory boards of EMD Serono, Merck and Pfizer. The other authors and consortia members declare no competing interests.
Figures
Similar articles
-
PD-L1 blockade with avelumab: A new paradigm for treating Merkel cell carcinoma.Cancer Biol Ther. 2017 Dec 2;18(12):937-939. doi: 10.1080/15384047.2017.1394552. Epub 2017 Nov 27. Cancer Biol Ther. 2017. PMID: 29172995 Free PMC article.
-
Immunotherapy for Merkel Cell Carcinoma.Curr Treat Options Oncol. 2018 Sep 20;19(11):57. doi: 10.1007/s11864-018-0574-5. Curr Treat Options Oncol. 2018. PMID: 30238195 Review.
-
[Immune checkpoint inhibition in Merkel cell carcinoma].Hautarzt. 2019 Sep;70(9):684-690. doi: 10.1007/s00105-019-4465-x. Hautarzt. 2019. PMID: 31468071 Review. German.
-
MHC class-I downregulation in PD-1/PD-L1 inhibitor refractory Merkel cell carcinoma and its potential reversal by histone deacetylase inhibition: a case series.Cancer Immunol Immunother. 2019 Jun;68(6):983-990. doi: 10.1007/s00262-019-02341-9. Epub 2019 Apr 16. Cancer Immunol Immunother. 2019. PMID: 30993371 Free PMC article.
-
Advances in Immunotherapy for Metastatic Merkel Cell Carcinoma: A Clinician's Guide.J Natl Compr Canc Netw. 2018 Jun;16(6):782-790. doi: 10.6004/jnccn.2018.7049. J Natl Compr Canc Netw. 2018. PMID: 29891528 Review.
Cited by
-
Clinical Features and Prognosis of Merkel Cell Carcinoma in Elderly Patients.Med Sci Monit. 2020 Jul 12;26:e924570. doi: 10.12659/MSM.924570. Med Sci Monit. 2020. PMID: 32653892 Free PMC article.
-
Merkel Cell Polyomavirus (MCPyV) and Cancers: Emergency Bell or False Alarm?Cancers (Basel). 2022 Nov 11;14(22):5548. doi: 10.3390/cancers14225548. Cancers (Basel). 2022. PMID: 36428641 Free PMC article. Review.
-
TRK Protein Expression in Merkel Cell Carcinoma Is Not Caused by NTRK Fusions.Int J Mol Sci. 2022 Dec 6;23(23):15366. doi: 10.3390/ijms232315366. Int J Mol Sci. 2022. PMID: 36499693 Free PMC article.
-
RB1 alteration and poor prognosis in women with high-grade neuroendocrine carcinoma of the uterine cervix: a NeCTuR study.J Gynecol Oncol. 2023 Jul;34(4):e50. doi: 10.3802/jgo.2023.34.e50. Epub 2023 Feb 9. J Gynecol Oncol. 2023. PMID: 36807750 Free PMC article.
-
Merkel cell carcinoma of the eyelid and periocular region: A review.Saudi J Ophthalmol. 2022 Apr 18;35(3):186-192. doi: 10.4103/SJOPT.SJOPT_55_21. eCollection 2021 Jul-Sep. Saudi J Ophthalmol. 2022. PMID: 35601863 Free PMC article.
References
-
- Toker C. Trabecular carcinoma of the skin. Arch. Dermatol. 1972;105:107–110. - PubMed
-
- Agelli M, Clegg LX, Becker JC, Rollison DE. The etiology and epidemiology of merkel cell carcinoma. Curr. Probl. Cancer. 2010;34:14–37. - PubMed
-
- Harms PW. Update on Merkel cell carcinoma. Clin. Lab. Med. 2017;37:485–501. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
