

Review
doi: 10.5152/dir.2018.18186.
Magnetic resonance elastography: basic principles, technique, and clinical applications in the liver
Affiliations
- PMID: 30272563
- PMCID: PMC6223825
- DOI: 10.5152/dir.2018.18186
Item in Clipboard
Review
Magnetic resonance elastography: basic principles, technique, and clinical applications in the liver
Diagn Interv Radiol.
2018 Nov.
Abstract
Magnetic resonance elastography (MRE) is a constantly advancing technique for assessment of stiffness of tissues with newer technology and sequences. It is being increasingly used for the assessment of liver fibrosis. In this article, we discuss the advantages of MRE over biopsy and noninvasive methods such as US elastography in the assessment of liver fibrosis. Image acquisition and interpretation of liver MRE is also discussed.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures

Disc-shaped passive driver. Its flat surface touching the patient is made of drum-like elastic membrane. Plastic connecting tube transports the acoustic wave originating from the generator, known as the active driver (not shown) which is located outside the MRI examination room, to the passive driver. Passive driver is placed over the liver and held in place by an elastic binder. Continuous low frequency (60 Hz) vibrations are delivered into the liver from the surface of lower rib cage.
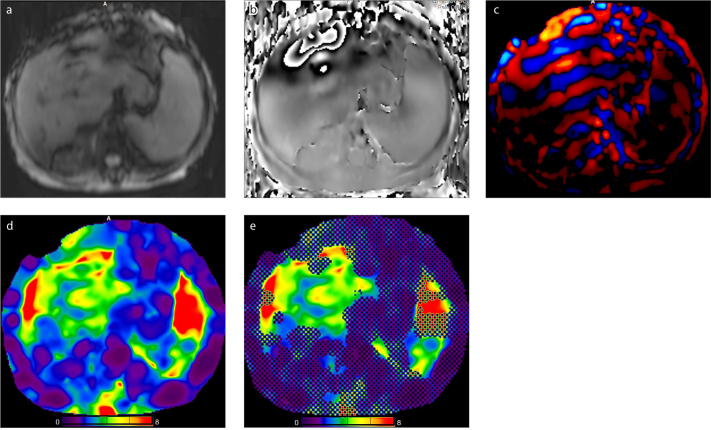
MRE images of a 68-year-old woman with chronic liver diasease. Magnitude image (a), phase image (b), wave image (c), color-coded elastogram (d), and confidence map (e). Liver tissue stiffness values are measured on confidence map by drawing largest possible ROIs on four different levels of liver. Cross-hatched regions on confidence map are areas of low-confidence data excluded by the processing algorithm. Nonparenchymal structures (i.e., large vessels, bile ducts, gall bladder) that will affect measurement should be avoided while drawing the ROI. The mean value and range of liver stiffness are reported in units of kPa. The mean hepatic stifness value in this patient is measured as 3.7 kPa (range, 2.80–4.33 kPa). Note also increased stiffness in the splenic parenchyma.
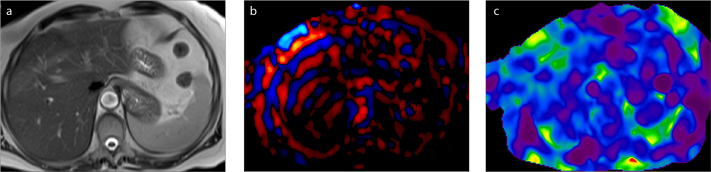
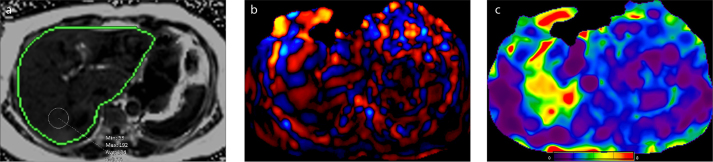
An 81-year-old woman with postcholecystectomy syndrome. T2-weighted image (a), wave image (b), and elastogram (c). Elastogram in this subject with a normal liver showed mean shear stiffness value of 2.27 kPa.

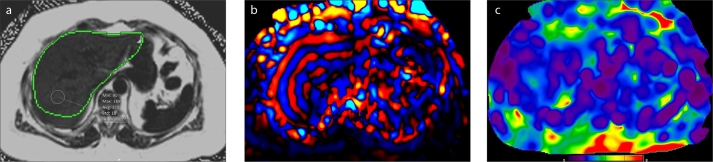
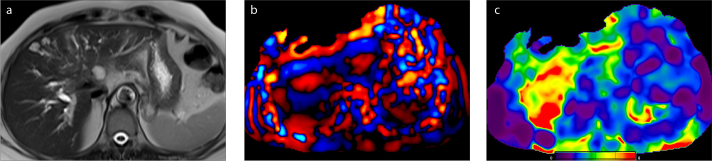
A 62-year-old woman with hepatitis B virus infection. T2-weighted image (a), wave image (b), and elastogram (c). Measurements from the elastogram revealed elevated stiffness values with a mean of 6.20 kPa consistent with Stage 4 fibrosis.
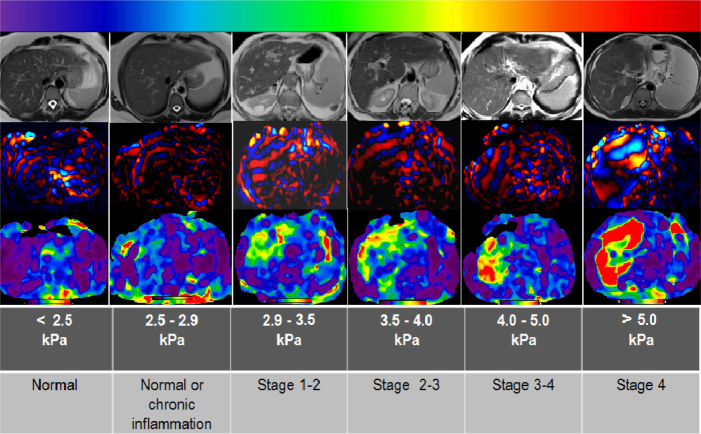
Relationship between MRE-measured stiffness of the liver and the stage of hepatic fibrosis. MRE can be used to stage fibrosis in various diffuse liver diseases. For example, in this figure, the patient with stage 1–2 fibrosis has primary biliary cirrhosis and the patient with stage 4 fibrosis has primary sclerosing cholangitis. The patients with stage 2–3 and 3–4 fibrosis have hepatitis B virus infection. In color-coded elastogram, relative tissue stiffness is shown on a color scale, ranging from softest (0 kPa; color-coded with purple) to hardest (8 kPa; color-coded with red). The stiffness values correlated with the stage of fibrosis that we used in this figure were obtained from Table 3 in Srinivasa Babu et al. (1).
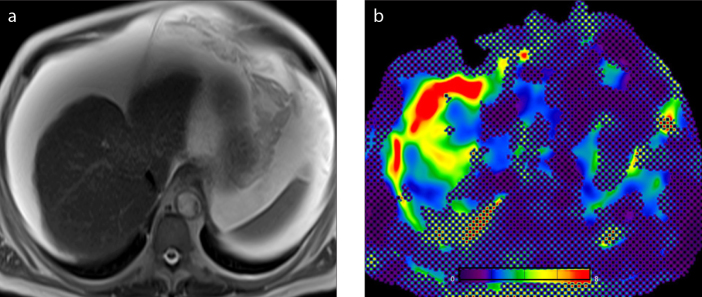
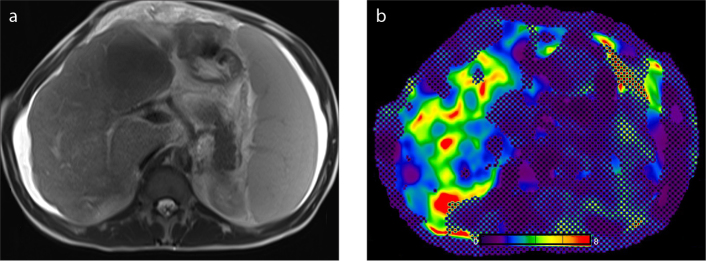
A 68-year-old man with chronic liver disease. T2-weighted image (a) shows atrophic liver and massive ascites. The presence of ascites did not seem to influence the data acquisition in this patient. Confidence map (b) outlines the hepatic areas with sufficient wave propagation. There is considerable amount of liver parenchyma outside the cross-hatching marks from which stiffness measurements can be made.
A 58-year-old man with Chilaiditi syndrome. T2-weighted image (a) shows a portion of the colon abnormally interposed between the liver and the diaphragm. The passive driver was shifted to left in order to optimize the delivery of the vibrations into the liver. Shear waves have adequate hepatic penetration in the left lobe. Normal hepatic stiffness (color-coded with blue) can be seen on confidence map (b).
A 55-year-old woman with nonalcoholic fatty liver disease. According to HISTO sequence analysis (MR spectroscopy not shown) and fat fraction parametric map (a), fat signal fraction rates are elevated, 13.2% and 12.9%, respectively. Panel (b) shows the wave image. Elastogram (c) determined mean stiffness as 2.22 kPa which is within normal limits. Simple steatosis does not have a significant effect on stiffness values.
A 58-year-old woman with nonalcoholic steatohepatitis (NASH). According to HISTO sequence analysis (MR spectroscopy not shown) and fat fraction map (a), fat signal fraction rates are 13.8% and 13.4%, respectively. Panel (b) shows the wave image and panel (c) shows the elastogram. This patient had a mean liver stiffness of 3.10 kPa (range, 2.25–4.49 kPa). Biopsy showed steatohepatitis index as: steatosis +++, and inflammation ++. Necroinflammatory activity in NASH increases the hepatic stiffness values.
A 31-year-old man with Budd-Chiari syndrome. T2-weighted image (a) shows atrophy of the right liver lobe, hepatic contour nodularity, splenomegaly, and ascites. Elastogram (b) revealed mean shear stiffness value of 2.95 kPa. Hepatic venous congestion is one of the confounders, which elevates liver stiffness and may lead to overestimation of fibrosis stage.
A 65-year-old woman with high cholestasis parameters. T2-weighted image (a) shows severe dilatation of intrahepatic bile ducts. Panel (b) shows wave image. Mean stiffness value of 5.20 kPa was obtained from the elastograms (c).

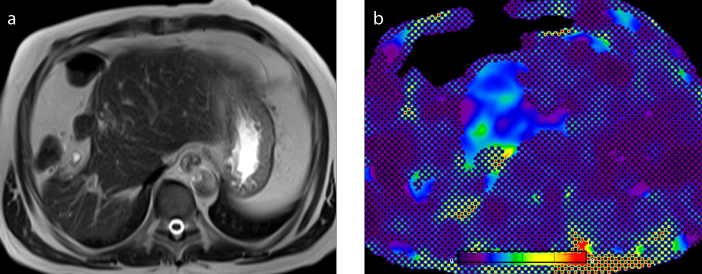
A 38-year-old man with biopsy-proven adenocarcinoma metastasis. T2-weighted image (a) shows a large heterogeneous mass with lobulated contours, measuring 20×14×12 cm at its widest part, and involving almost all of the right lobe of the liver. Elastogram (b) reveals high shear stiffness (6.7 kPa; color-coded with red) within the tumor.
Similar articles
-
Magnetic Resonance Elastography of Liver: Current Update.Top Magn Reson Imaging. 2018 Oct;27(5):319-333. doi: 10.1097/RMR.0000000000000177. Top Magn Reson Imaging. 2018. PMID: 30289828 Free PMC article. Review.
-
Liver MR Elastography Technique and Image Interpretation: Pearls and Pitfalls.Radiographics. 2019 Nov-Dec;39(7):1983-2002. doi: 10.1148/rg.2019190034. Epub 2019 Oct 18. Radiographics. 2019. PMID: 31626569 Review.
-
Assessment of advanced hepatic MR elastography methods for susceptibility artifact suppression in clinical patients.J Magn Reson Imaging. 2018 Apr;47(4):976-987. doi: 10.1002/jmri.25818. Epub 2017 Aug 11. J Magn Reson Imaging. 2018. PMID: 28801939 Free PMC article.
-
Magnetic resonance elastography (MRE) in cancer: Technique, analysis, and applications.Prog Nucl Magn Reson Spectrosc. 2015 Nov;90-91:32-48. doi: 10.1016/j.pnmrs.2015.06.001. Epub 2015 Jun 23. Prog Nucl Magn Reson Spectrosc. 2015. PMID: 26592944 Free PMC article. Review.
-
MR elastography for noninvasive assessment of hepatic fibrosis: reproducibility of the examination and reproducibility and repeatability of the liver stiffness value measurement.J Magn Reson Imaging. 2014 Feb;39(2):326-31. doi: 10.1002/jmri.24147. Epub 2013 Apr 15. J Magn Reson Imaging. 2014. PMID: 23589232
Cited by
-
Quantitative MRI of diffuse liver diseases: techniques and tissue-mimicking phantoms.MAGMA. 2023 Aug;36(4):529-551. doi: 10.1007/s10334-022-01053-z. Epub 2022 Dec 14. MAGMA. 2023. PMID: 36515810 Review.
-
Photoacoustic imaging as a tool to probe the tumour microenvironment.Dis Model Mech. 2019 Jul 16;12(7):dmm039636. doi: 10.1242/dmm.039636. Dis Model Mech. 2019. PMID: 31337635 Free PMC article. Review.
-
Liver surface nodularity on non-contrast MRI identifies advanced fibrosis in patients with NAFLD.Eur Radiol. 2022 Mar;32(3):1781-1791. doi: 10.1007/s00330-021-08261-6. Epub 2021 Sep 17. Eur Radiol. 2022. PMID: 34533606
-
A portable single-sided magnetic-resonance sensor for the grading of liver steatosis and fibrosis.Nat Biomed Eng. 2021 Mar;5(3):240-251. doi: 10.1038/s41551-020-00638-0. Epub 2020 Nov 30. Nat Biomed Eng. 2021. PMID: 33257853
-
Multi-frequency magnetic resonance elastography of the pancreas: measurement reproducibility and variance among healthy volunteers.Gastroenterol Rep (Oxf). 2022 Jul 29;10:goac033. doi: 10.1093/gastro/goac033. eCollection 2022. Gastroenterol Rep (Oxf). 2022. PMID: 35910246 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
