

Familial Multiple Cavernous Malformation Syndrome: MR Features in This Uncommon but Silent Threat
- PMID: 30151459
- PMCID: PMC6100658
- DOI: 10.5334/jbr-btr.938
Familial Multiple Cavernous Malformation Syndrome: MR Features in This Uncommon but Silent Threat
Abstract
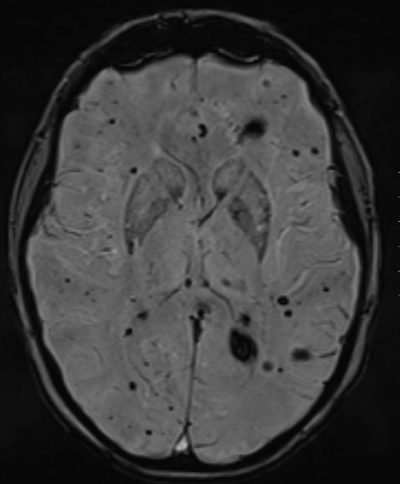
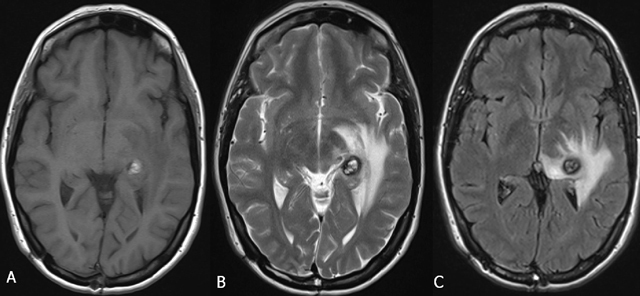
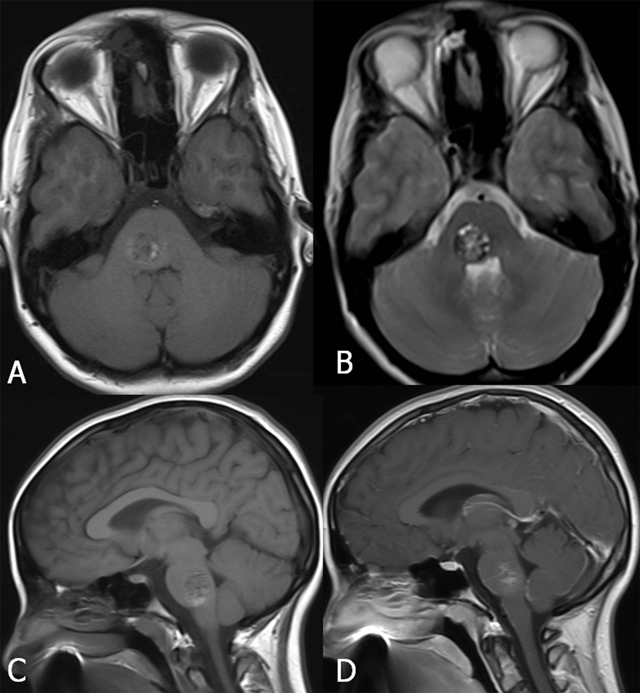
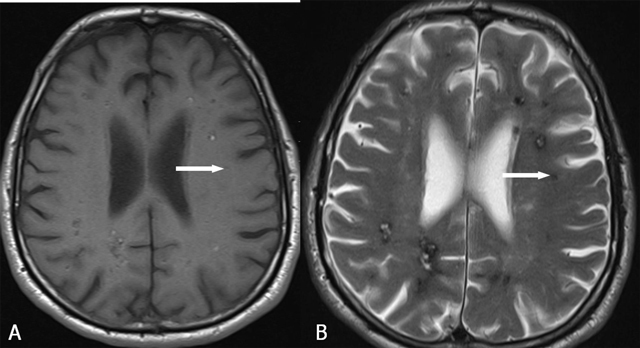
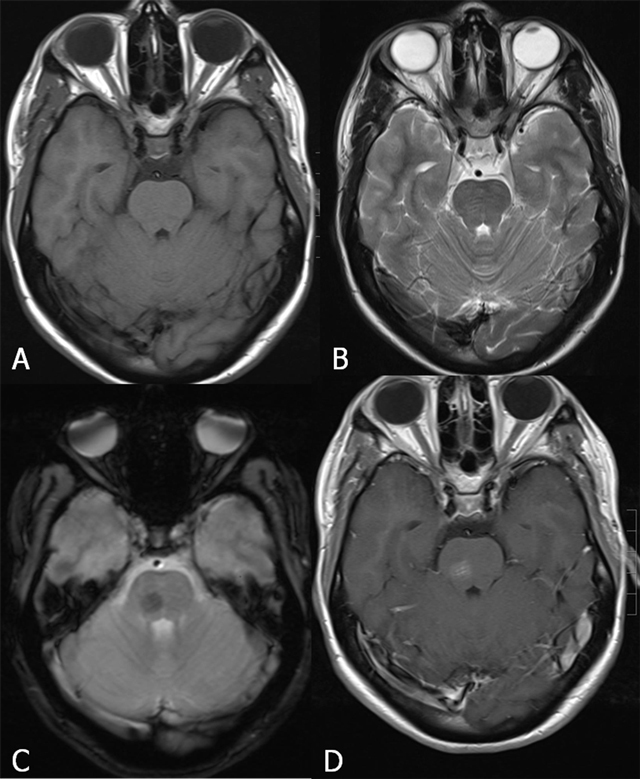
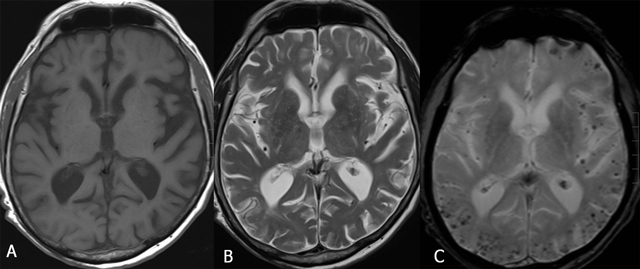
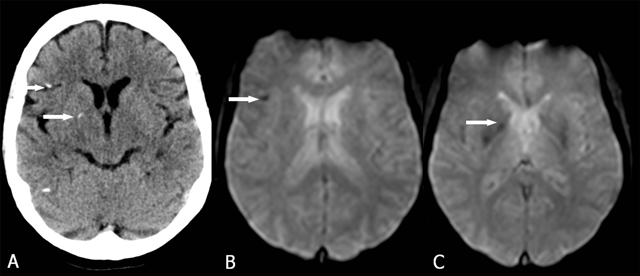
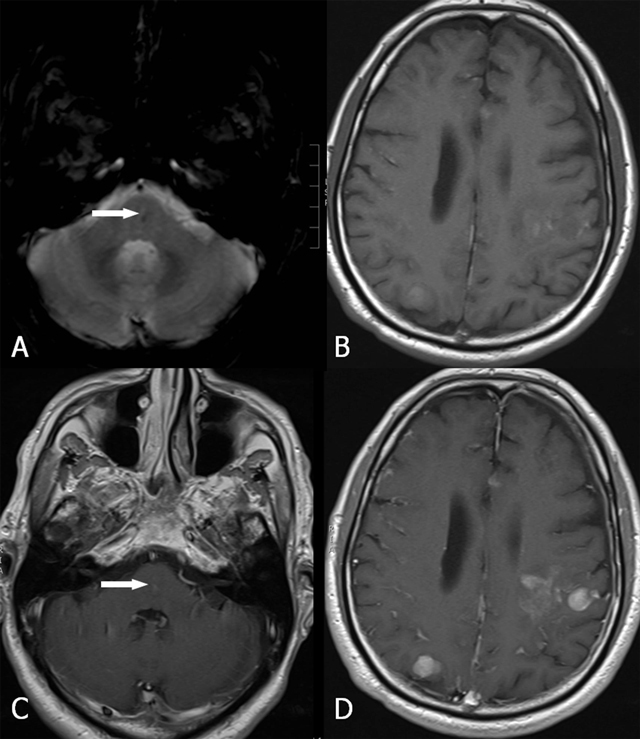
Cerebral cavernous malformations (CCM) are vascular malformations in the brain and spinal cord. The familial form of cerebral cavernous malformation (FCCM) is uncommon. This autosomal dominant pathology mostly presents with seizures and focal neurological symptoms. Many persons affected by FCCM remain asymptomatic. However, acute hemorrhages may appear over time. MRI demonstrates multiple focal regions of susceptibility induced signal loss, well seen on gradient-echo sequences (GRE) or even better on susceptibility-weighted imaging (SWI). The presence of a single CCM - especially in young persons - without history of FCCM does not exclude this diagnosis. Some clinicians also advise an MRI of the spinal cord at the time of diagnosis to serve as a baseline and a control MRI of the brain every one to two years. MRI is certainly indicated in individuals with obvious new neurologic symptoms. Symptomatic siblings should also undergo an MRI of the brain to determine presence, size, and location of the lesions. Even in asymptomatic siblings, a screening MRI may be considered, as there may be an increased risk of hemorrhage, spontaneous or due to the use of certain medications; the knowledge of the presence and the type of these lesions are important. Surgical removal of a CCM may be justified to prevent a life-threatening hemorrhage. Control MRI may reveal the postoperative outcome.
Keywords: Cerebral cavernous malformation; Familial cerebral cavernous malformation syndrome; MRI.
Figures







Similar articles
-
Familial Cerebral Cavernous Malformations.2003 Feb 24 [updated 2023 Jul 27]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2024. 2003 Feb 24 [updated 2023 Jul 27]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2024. PMID: 20301470 Free Books & Documents. Review.
-
Accuracy of SWI sequences compared to T2*-weighted gradient echo sequences in the detection of cerebral cavernous malformations in the familial form.Neuroradiol J. 2016 Oct;29(5):326-35. doi: 10.1177/1971400916665376. Epub 2016 Aug 22. Neuroradiol J. 2016. PMID: 27549150 Free PMC article.
-
Multiple cerebral cavernous malformations: Clinical course of confirmed, assumed and non-familial disease.Eur J Neurol. 2022 May;29(5):1427-1434. doi: 10.1111/ene.15253. Epub 2022 Feb 3. Eur J Neurol. 2022. PMID: 35060255
-
The value of T(2) (*)-weighted gradient echo imaging for detection of familial cerebral cavernous malformation: A study of two families.Exp Ther Med. 2013 Feb;5(2):448-452. doi: 10.3892/etm.2012.845. Epub 2012 Nov 30. Exp Ther Med. 2013. PMID: 23408355 Free PMC article.
-
[Diagnostic imaging of hemangiomas in the brain].Brain Nerve. 2011 Jan;63(1):5-15. Brain Nerve. 2011. PMID: 21228443 Review. Japanese.
Cited by
-
Multiple Cavernous Malformation Syndrome in an Infant: A Case Report.Cureus. 2024 Jul 3;16(7):e63750. doi: 10.7759/cureus.63750. eCollection 2024 Jul. Cureus. 2024. PMID: 39100028 Free PMC article.
-
Genotype-phenotype correlations in multiple lesions of familial cerebral cavernous malformations concerning phosphatidylinositol 3-kinase catalytic subunit alpha mutations.Clin Transl Med. 2024 Mar;14(3):e1610. doi: 10.1002/ctm2.1610. Clin Transl Med. 2024. PMID: 38450890 Free PMC article. No abstract available.
-
Advances in Mass Spectrometry of Gangliosides Expressed in Brain Cancers.Int J Mol Sci. 2024 Jan 22;25(2):1335. doi: 10.3390/ijms25021335. Int J Mol Sci. 2024. PMID: 38279335 Free PMC article. Review.
-
Clinicoradiologic data of familial cerebral cavernous malformation with age-related disease burden.Ann Clin Transl Neurol. 2023 Mar;10(3):373-383. doi: 10.1002/acn3.51728. Epub 2023 Jan 11. Ann Clin Transl Neurol. 2023. PMID: 36629374 Free PMC article.
-
Magnetic Resonance Imaging of Multiple Cerebral and Spinal Cavernous Malformations of a Patient with Dementia and Tetraparesis.Diagnostics (Basel). 2022 Mar 10;12(3):677. doi: 10.3390/diagnostics12030677. Diagnostics (Basel). 2022. PMID: 35328230 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
