

Determinants of the Nasal Microbiome: Pilot Study of Effects of Intranasal Medication Use
- PMID: 30128169
- PMCID: PMC6088474
- DOI: 10.1177/2152656718789519
Determinants of the Nasal Microbiome: Pilot Study of Effects of Intranasal Medication Use
Abstract
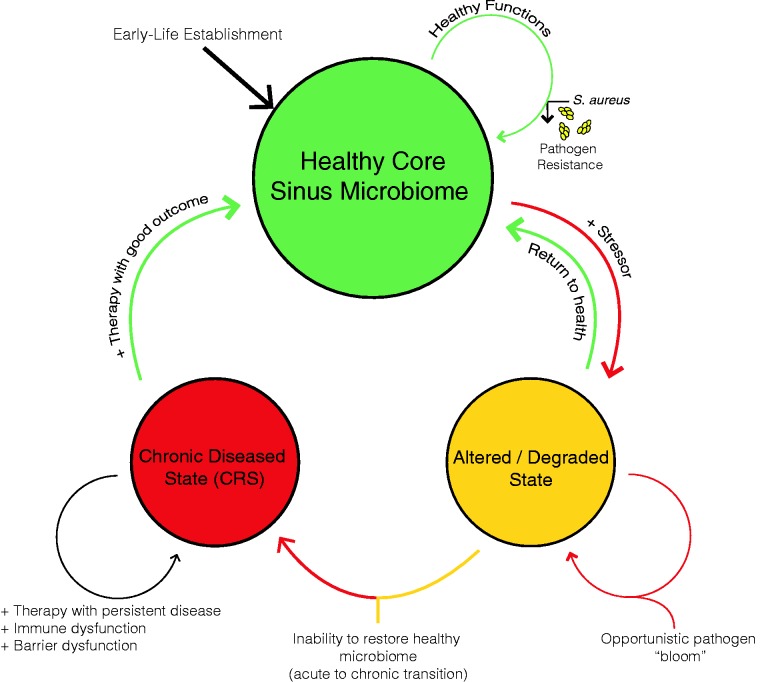
Introduction: A role for bacteria and other microbes has long been suspected in the chronic inflammatory sinonasal diseases. Recent studies utilizing culture-independent, sequence-based identification have demonstrated aberrant shifts in the sinus microbiota of chronic rhinosinusitis subjects, compared with ostensibly healthy controls. Examining how such microbiota shifts occur and the potential for physician-prescribed interventions to influence microbiota dynamics are the topics of the current article.
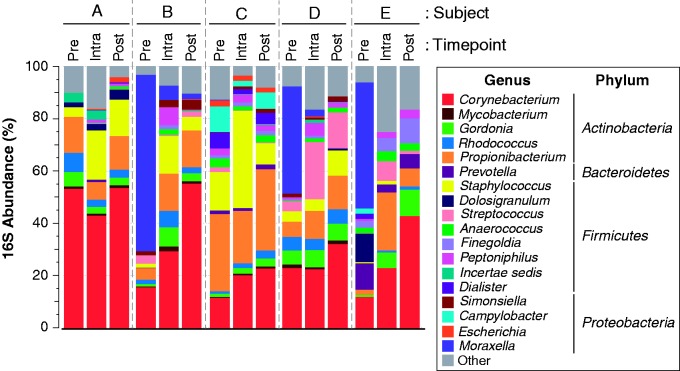
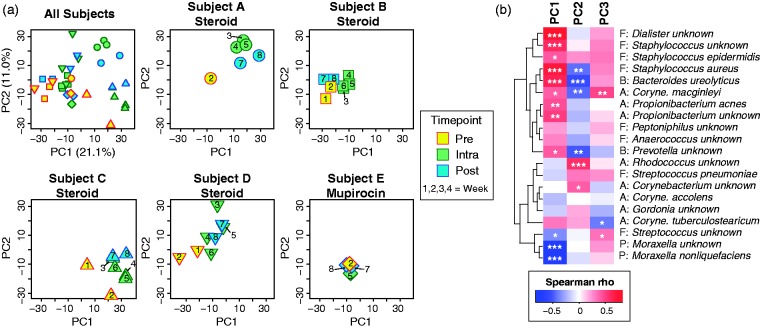
Methods: The nasal cavity microbiota of 5 subjects was serially examined over an 8-week period using pan-bacterial 16S rRNA gene sequencing. Four of the subjects were administered topical mometasone furoate spray, while 1 subject underwent a mupirocin decolonization procedure in anticipation of orthopedic surgery.
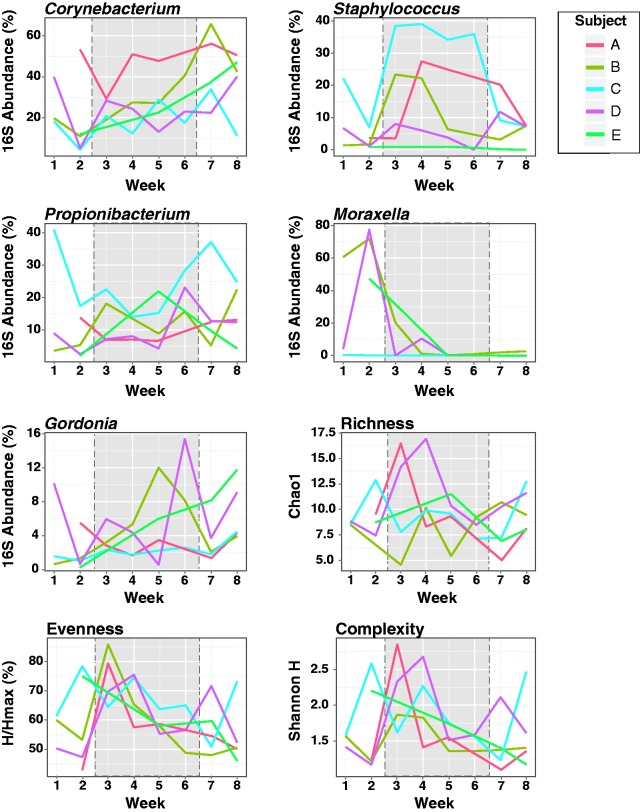
Results: Measures of microbial diversity were unaffected by intranasal treatment in 2 patients and were markedly increased in the remaining 3. The increase in microbial diversity was related to clearance of Moraxella spp. and a simultaneous increase in members of the phylum Actinobacteria. Both effects persisted at least 2 weeks beyond cessation of treatment. Transient changes in the relative abundance of several bacterial genera, including Staphylococcus and Priopionibacteria, were also observed during treatment.
Conclusions: The effects of intranasal steroids on the sinonasal microbiome are poorly understood, despite their widespread use in treating chronic sinonasal inflammatory disorders. In this longitudinal study, administration of intranasal mometasone furoate or mupirocin resulted in shifts in microbial diversity that persisted to some degree following treatment cessation. Further characterization of these effects as well as elucidation of the mechanism(s) underlying these changes is needed.
Keywords: anterior nares; bacteria; microbiome; nasal steroid; rhinitis; sinusitis.
Figures
Similar articles
-
The influence of nasal bacterial microbiome diversity on the pathogenesis and prognosis of chronic rhinosinusitis patients with polyps.Eur Arch Otorhinolaryngol. 2021 Apr;278(4):1075-1088. doi: 10.1007/s00405-020-06370-4. Epub 2020 Sep 22. Eur Arch Otorhinolaryngol. 2021. PMID: 32960349
-
Impact of saline irrigation and topical corticosteroids on the postsurgical sinonasal microbiota.Int Forum Allergy Rhinol. 2015 Mar;5(3):185-90. doi: 10.1002/alr.21467. Epub 2014 Dec 29. Int Forum Allergy Rhinol. 2015. PMID: 25556553 Free PMC article.
-
Mapping and comparing bacterial microbiota in the sinonasal cavity of healthy, allergic rhinitis, and chronic rhinosinusitis subjects.Int Forum Allergy Rhinol. 2017 Jun;7(6):561-569. doi: 10.1002/alr.21934. Epub 2017 May 8. Int Forum Allergy Rhinol. 2017. PMID: 28481057
-
Mometasone furoate nasal spray: a systematic review.Multidiscip Respir Med. 2016 May 2;11:18. doi: 10.1186/s40248-016-0054-3. eCollection 2016. Multidiscip Respir Med. 2016. PMID: 27141307 Free PMC article. Review.
-
[Intranasal steroid therapy in inflammatory nasal-sinus pathology in pediatric age].Minerva Pediatr. 2009 Jun;61(3):323-31. Minerva Pediatr. 2009. PMID: 19461575 Review. Italian.
Cited by
-
Acute SARS-CoV-2 infection is associated with an increased abundance of bacterial pathogens, including Pseudomonas aeruginosa in the nose.Cell Rep. 2021 Aug 31;36(9):109637. doi: 10.1016/j.celrep.2021.109637. Epub 2021 Aug 13. Cell Rep. 2021. PMID: 34433082 Free PMC article.
-
Nasal microbiome disruption and recovery after mupirocin treatment in Staphylococcus aureus carriers and noncarriers.Sci Rep. 2022 Nov 17;12(1):19738. doi: 10.1038/s41598-022-21453-4. Sci Rep. 2022. PMID: 36396730 Free PMC article.
-
The microbiome of the upper respiratory tract in health and disease.BMC Biol. 2019 Nov 7;17(1):87. doi: 10.1186/s12915-019-0703-z. BMC Biol. 2019. PMID: 31699101 Free PMC article. Review.
-
The Effects of Corticosteroids on the Respiratory Microbiome: A Systematic Review.Front Med (Lausanne). 2021 Mar 10;8:588584. doi: 10.3389/fmed.2021.588584. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33777968 Free PMC article.
-
COVID-19 and upper respiratory tract: Collecting swab specimens from patients inhaling corticosteroids.J Allergy Clin Immunol. 2020 Dec;146(6):1457. doi: 10.1016/j.jaci.2020.09.004. Epub 2020 Sep 29. J Allergy Clin Immunol. 2020. PMID: 33019963 Free PMC article. No abstract available.
References
-
- Brozek JL, Bousquet J, Baena-Cagnani CE, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol. 2010; 126:466–476. - PubMed
-
- Bousquet J, Fokkens W, Burney P, et al. Important research questions in allergy and related diseases: nonallergic rhinitis: a GA2LEN paper. Allergy. 2008; 63:842–853. - PubMed
-
- Ramakrishnan VR. Pharmacotherapy for nonallergic rhinitis In: Meyers AD, ed. Otolaryngology & Facial Plastic Surgery. eMedicine from Medscape; https://emedicine.medscape.com/article/874171-overview
-
- Van Gerven L, Boeckxstaens G, Hellings P. Up-date on neuro-immune mechanisms involved in allergic and non-allergic rhinitis. Rhinology, 2012; 50:227–235. - PubMed
-
- Orlandi RR, Kingdom TT, Hwang PH, et al. International consensus statement on allergy and rhinology: rhinosinusitis. Int Forum Allergy Rhinol. 2016; 6(Suppl 1):S22–S209. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
