

Is Visible Aminolevulinic Acid-Induced Fluorescence an Independent Biomarker for Prognosis in Histologically Confirmed (World Health Organization 2016) Low-Grade Gliomas?
- PMID: 30107580
- PMCID: PMC6537633
- DOI: 10.1093/neuros/nyy365
Is Visible Aminolevulinic Acid-Induced Fluorescence an Independent Biomarker for Prognosis in Histologically Confirmed (World Health Organization 2016) Low-Grade Gliomas?
Abstract
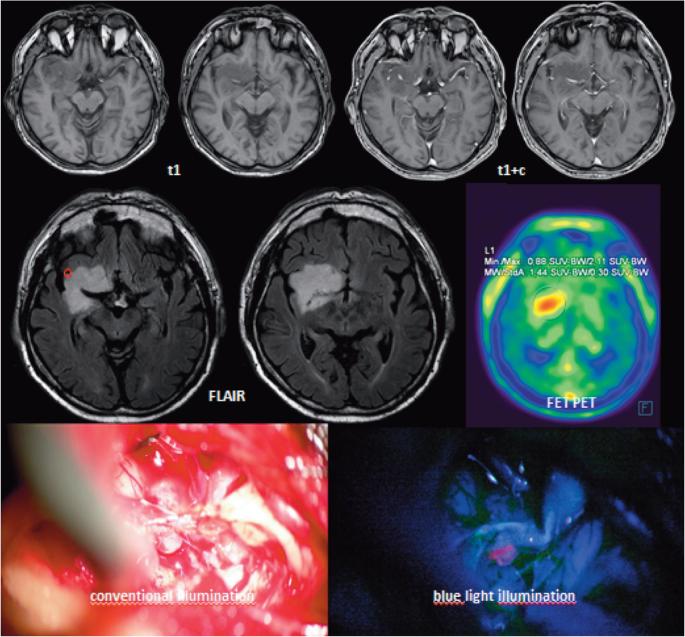
Background: Approximately 20% of low-grade gliomas (LGG) display visible protoporphyrin fluorescence during surgery after 5-aminolevulinic acid (5-ALA) administration.
Objective: To determine if fluorescence represents a prognostic marker in LGG.
Methods: Seventy-four consecutive patients with LGG (World Health Organization 2016) were operated on with 5-ALA. Fluorescent tissue was specifically biopsied. Tumor size, age, Karnofsky index, contrast-enhancement, fluorescence, and molecular factors (IDH1/IDH2-mutations, Ki67/MIB1 Index, 1p19q codeletions, ATRX, EGFR, p53 expression, and O6-methylguanine DNA methyltransferase promotor methylation), were related to progression-free survival (PFS), malignant transformation-free survival (MTFS) and overall survival (OS).
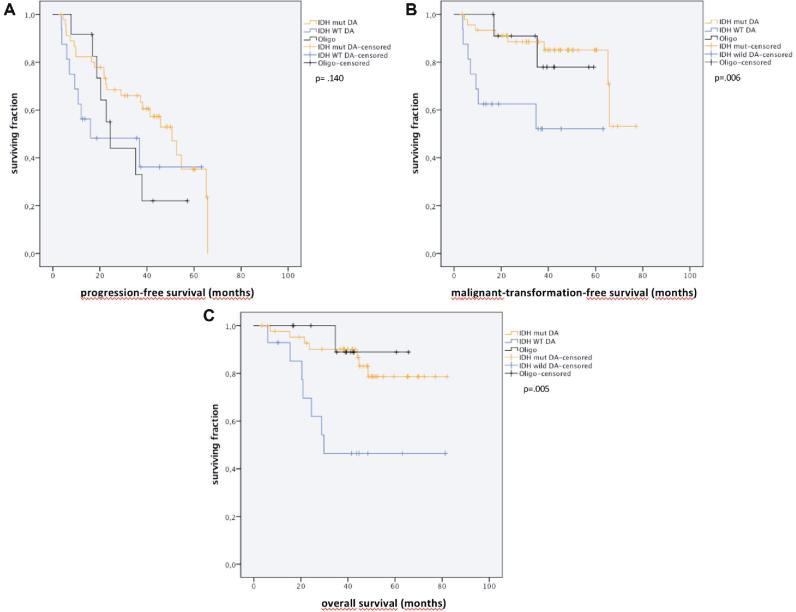
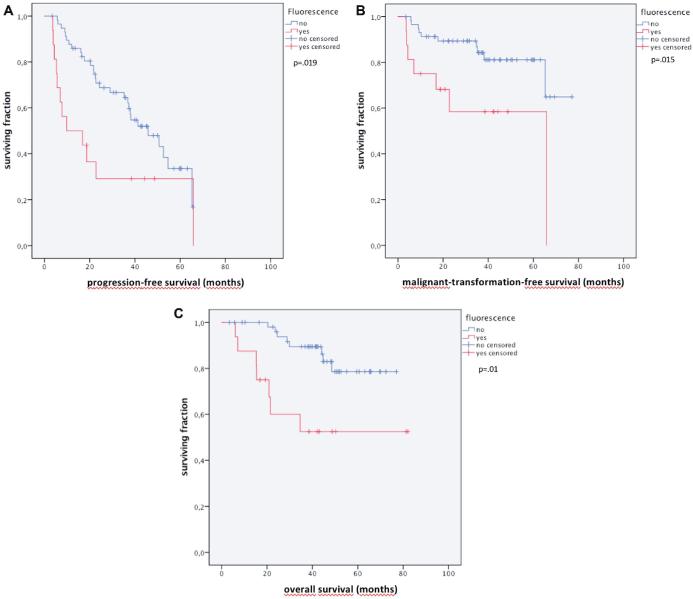
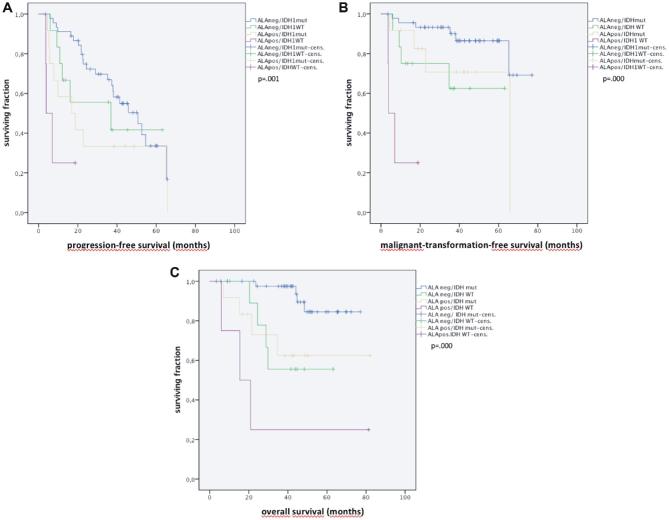
Results: Sixteen of seventy-four LGGs (21.6%) fluoresced. Fluorescence was partially related to weak enhancement on magnetic resonance imaging and increased (positron emission tomography)PET-FET uptake, but not to Karnofsky Performance Score, tumor size, or age. Regarding molecular markers, only EGFR expression differed marginally (fluorescing vs nonfluorescing: 19% vs 5%; P = .057). Median follow-up was 46.4 mo (95% confidence interval [CI]: 41.8-51.1). PFS, MTFS, and OS were shorter in fluorescing tumors (PFS: median 9.8 mo, 95% CI: 1.00-27.7 vs 45.8, 31.9-59.7, MTFS: 43.0 [27.5-58.5] vs 64.6 [57.7-71.5], median not reached, P = .015; OS: 51.6, [34.8-68.3] vs [68.2, 62.7-73.8], P = .002). IDH mutations significantly predicted PFS, MTFS, and OS. In multivariate analysis IDH status and fluorescence both independently predicted MTFS and OS. PFS was not independently predicted by fluorescence.
Conclusion: This is the first report investigating the role of ALA-induced fluorescence in histologically confirmed LGG. Fluorescence appeared to be a marker for inherent malignant transformation and OS, independently of known prognostic markers. Fluorescence in LGG might be taken into account when deciding on adjuvant therapies.
Keywords: 5-ALA; Diffuse astrocytoma; Fuorescence-guided resection; Low-grade glioma; Malignization transformation-free survival (MTFS); PET.
© Congress of Neurological Surgeons 2018.
Figures
Similar articles
-
CD34 microvascularity in low-grade glioma: correlation with 5-aminolevulinic acid fluorescence and patient prognosis in a multicenter study at three specialized centers.J Neurosurg. 2022 Sep 16;138(5):1281-1290. doi: 10.3171/2022.7.JNS22921. Print 2023 May 1. J Neurosurg. 2022. PMID: 36115057
-
The Value of 5-Aminolevulinic Acid in Low-grade Gliomas and High-grade Gliomas Lacking Glioblastoma Imaging Features: An Analysis Based on Fluorescence, Magnetic Resonance Imaging, 18F-Fluoroethyl Tyrosine Positron Emission Tomography, and Tumor Molecular Factors.Neurosurgery. 2016 Mar;78(3):401-11; discussion 411. doi: 10.1227/NEU.0000000000001020. Neurosurgery. 2016. PMID: 26366972 Free PMC article.
-
Fluorescence real-time kinetics of protoporphyrin IX after 5-ALA administration in low-grade glioma.J Neurosurg. 2021 Jun 18;136(1):9-15. doi: 10.3171/2020.10.JNS202881. Print 2022 Jan 1. J Neurosurg. 2021. PMID: 34144512
-
Molecular features assisting in diagnosis, surgery, and treatment decision making in low-grade gliomas.Neurosurg Focus. 2015 Mar;38(3):E2. doi: 10.3171/2015.1.FOCUS14745. Neurosurg Focus. 2015. PMID: 25727224 Review.
-
Selective 5-aminolevulinic acid-induced protoporphyrin IX fluorescence in Gliomas.Acta Neurochir (Wien). 2016 Oct;158(10):1935-41. doi: 10.1007/s00701-016-2897-y. Epub 2016 Aug 6. Acta Neurochir (Wien). 2016. PMID: 27496021 Review.
Cited by
-
5-ALA in Suspected Low-Grade Gliomas: Current Role, Limitations, and New Approaches.Front Oncol. 2021 Jul 30;11:699301. doi: 10.3389/fonc.2021.699301. eCollection 2021. Front Oncol. 2021. PMID: 34395266 Free PMC article. Review.
-
Systematic review-Time to malignant transformation in low-grade gliomas: Predicting a catastrophic event with clinical, neuroimaging, and molecular markers.Neurooncol Adv. 2021 Jul 27;3(1):vdab101. doi: 10.1093/noajnl/vdab101. eCollection 2021 Jan-Dec. Neurooncol Adv. 2021. PMID: 34466805 Free PMC article. Review.
-
Fluorescence Lifetime Imaging and Spectroscopic Co-Validation for Protoporphyrin IX-Guided Tumor Visualization in Neurosurgery.Front Oncol. 2021 Sep 14;11:741303. doi: 10.3389/fonc.2021.741303. eCollection 2021. Front Oncol. 2021. PMID: 34595120 Free PMC article.
-
5-Aminolevulinic Acid-A Biomarker for Worse Prognosis in IDH-Wildtype II Tumors? Evolution of a Fluorescence-Positive Diffuse Astrocytoma: A Case Report.J Neurol Surg Rep. 2022 Aug 25;83(3):e95-e99. doi: 10.1055/a-1858-7628. eCollection 2022 Jul. J Neurol Surg Rep. 2022. PMID: 36032798 Free PMC article.
-
Lower-grade gliomas surgery guided by GRPR-targeting PET/NIR dual-modality image probe: a prospective and single-arm clinical trial.Theranostics. 2024 Jan 1;14(2):819-829. doi: 10.7150/thno.91554. eCollection 2024. Theranostics. 2024. PMID: 38169486 Free PMC article. Clinical Trial.
References
-
- Aldave G, Tejada S, Pay E et al. .. Prognostic value of residual fluorescent tissue in glioblastoma patients after gross total resection in 5-aminolevulinic Acid-guided surgery. Neurosurgery. 2013;72(6):915-921. - PubMed
-
- Díez Valle R, Tejada Solis S, Idoate Gastearena MA, García de Eulate R, Domínguez Echávarri P, Aristu Mendiroz J. Surgery guided by 5-aminolevulinic fluorescence in glioblastoma: volumetric analysis of extent of resection in single-center experience. J Neurooncol. 2011;102(1):105-113. - PubMed
-
- Floeth FW, Pauleit D, Wittsack HJ et al. .. Multimodal metabolic imaging of cerebral gliomas: positron emission tomography with [18F]fluoroethyl-L-tyrosine and magnetic resonance spectroscopy. J Neurosurg. 2005;102(2):318-327. - PubMed
-
- Lau D, Hervey-Jumper SL, Chang S et al. .. A prospective phase II clinical trial of 5-aminolevulinic acid to assess the correlation of intraoperative fluorescence intensity and degree of histologic cellularity during resection of high-grade gliomas. J Neurosurgery. 2016;124(5):1300-1309. - PubMed
-
- Morshed RA, Han SJ, Lau D, Berger MS: Wavelength-specific lighted suction instrument for 5-aminolevulinic acid fluorescence-guided resection of deep-seated malignant glioma: technical note. J Neurosurg. 2018;128(5):1448-1453. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
