

The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review
- PMID: 30081871
- PMCID: PMC6090747
- DOI: 10.1186/s12889-018-5806-x
The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review
Abstract
Background: The evidence on the economic burden of cardiovascular disease (CVD) in low- and middle- income countries (LMICs) remains scarce. We conducted a comprehensive systematic review to establish the magnitude and knowledge gaps in relation to the economic burden of CVD and hypertension on households, health systems and the society.
Methods: We included studies using primary or secondary data to produce original economic estimates of the impact of CVD. We searched sixteen electronic databases from 1990 onwards without language restrictions. We appraised the quality of included studies using a seven-question assessment tool.
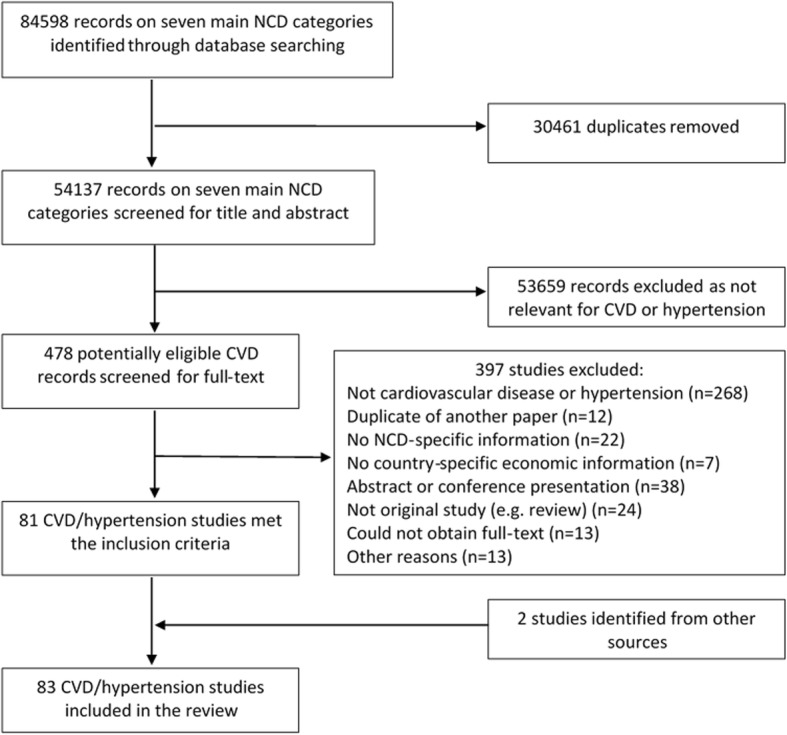
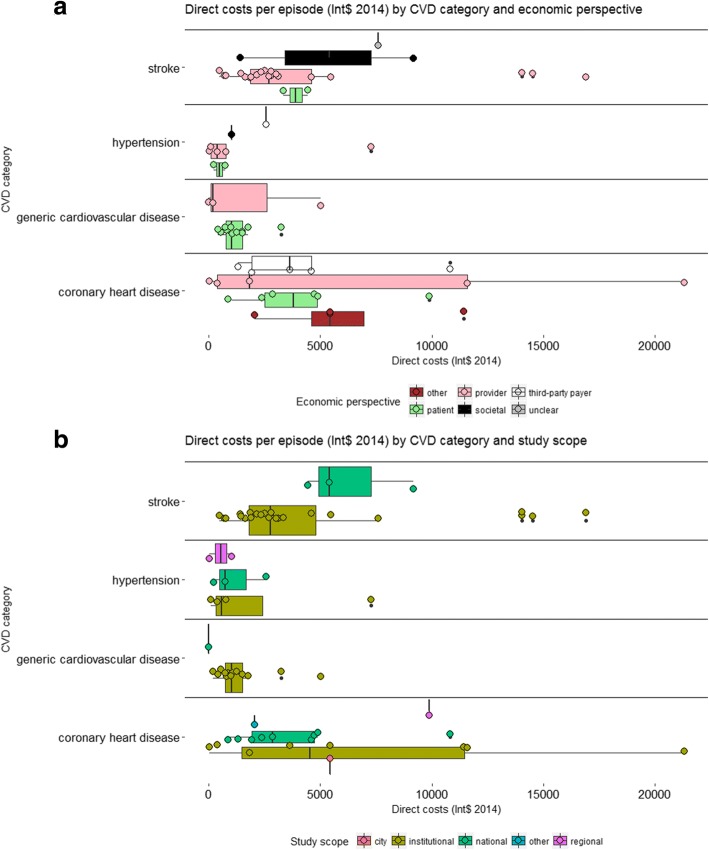
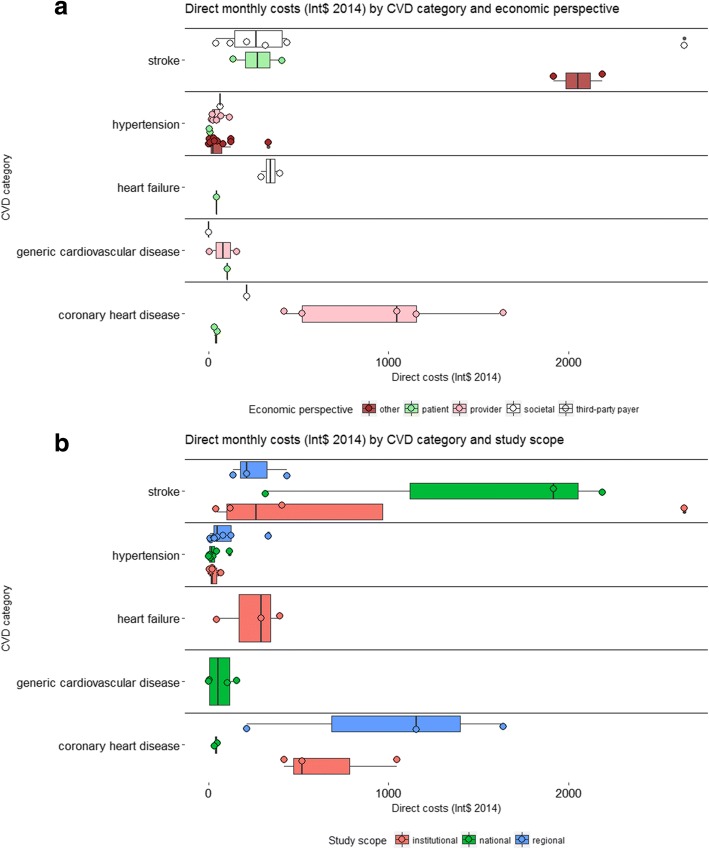
Results: Eighty-three studies met the inclusion criteria, most of which were single centre retrospective cost studies conducted in secondary care settings. Studies in China, Brazil, India and Mexico contributed together 50% of the total number of economic estimates identified. The quality of the included studies was generally low. Reporting transparency, particularly for cost data sources and results, was poor. The costs per episode for hypertension and generic CVD were fairly homogeneous across studies; ranging between $500 and $1500. In contrast, for coronary heart disease (CHD) and stroke cost estimates were generally higher and more heterogeneous, with several estimates in excess of $5000 per episode. The economic perspective and scope of the study appeared to impact cost estimates for hypertension and generic CVD considerably less than estimates for stroke and CHD. Most studies reported monthly costs for hypertension treatment around $22. Average monthly treatment costs for stroke and CHD ranged between $300 and $1000, however variability across estimates was high. In most LMICs both the annual cost of care and the cost of an acute episode exceed many times the total health expenditure per capita.
Conclusions: The existing evidence on the economic burden of CVD in LMICs does not appear aligned with policy priorities in terms of research volume, pathologies studied and methodological quality. Not only is more economic research needed to fill the existing gaps, but research quality needs to be drastically improved. More broadly, national-level studies with appropriate sample sizes and adequate incorporation of indirect costs need to replace small-scale, institutional, retrospective cost studies.
Keywords: Cardiovascular disease; Economic burden; Hypertension; Low-income; Middle-income; Non-communicable disease; Systematic review.
Conflict of interest statement
Not applicable.
Not applicable.
The author(s) declare that they have no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
The Economic Costs of Type 2 Diabetes: A Global Systematic Review.Pharmacoeconomics. 2015 Aug;33(8):811-31. doi: 10.1007/s40273-015-0268-9. Pharmacoeconomics. 2015. PMID: 25787932 Free PMC article. Review.
-
The global impact of non-communicable diseases on households and impoverishment: a systematic review.Eur J Epidemiol. 2015 Mar;30(3):163-88. doi: 10.1007/s10654-014-9983-3. Epub 2014 Dec 21. Eur J Epidemiol. 2015. PMID: 25527371 Review.
-
The global impact of non-communicable diseases on healthcare spending and national income: a systematic review.Eur J Epidemiol. 2015 Apr;30(4):251-77. doi: 10.1007/s10654-014-9984-2. Epub 2015 Jan 18. Eur J Epidemiol. 2015. PMID: 25595318 Review.
-
Cost of illness for childhood diarrhea in low- and middle-income countries: a systematic review of evidence and modelled estimates.BMC Public Health. 2020 May 5;20(1):619. doi: 10.1186/s12889-020-08595-8. BMC Public Health. 2020. PMID: 32370763 Free PMC article.
-
Economic Burden of Multiple Sclerosis in Low- and Middle-Income Countries: A Systematic Review.Pharmacoeconomics. 2021 Jul;39(7):789-807. doi: 10.1007/s40273-021-01032-7. Epub 2021 May 6. Pharmacoeconomics. 2021. PMID: 33956330 Free PMC article.
Cited by
-
The impact of health insurance on hypertension care: a household fixed effects study in India.BMC Public Health. 2024 Aug 22;24(1):2287. doi: 10.1186/s12889-024-19759-1. BMC Public Health. 2024. PMID: 39175008 Free PMC article.
-
Real-world evidence study on the impact of SPECT MPI, PET MPI, cCTA and stress echocardiography on downstream healthcare utilisation in patients with coronary artery disease in the US.BMC Cardiovasc Disord. 2024 Oct 9;24(1):543. doi: 10.1186/s12872-024-04225-y. BMC Cardiovasc Disord. 2024. PMID: 39379835 Free PMC article.
-
Modifiable and Non-modifiable Factors Associated with Low Awareness of Hypertension Treatment in Indonesia: A Cross-Sectional Population-Based National Survey.Glob Heart. 2022 Aug 16;17(1):56. doi: 10.5334/gh.1143. eCollection 2022. Glob Heart. 2022. PMID: 36051316 Free PMC article.
-
The effect of high blood pressure-health literacy, self-management behavior, self-efficacy and social support on the health-related quality of life of Kazakh hypertension patients in a low-income rural area of China: a structural equation model.BMC Public Health. 2021 Jun 10;21(1):1114. doi: 10.1186/s12889-021-11129-5. BMC Public Health. 2021. PMID: 34112122 Free PMC article.
-
Modelling the effect of compliance with WHO salt recommendations on cardiovascular disease mortality and costs in Brazil.PLoS One. 2020 Jul 9;15(7):e0235514. doi: 10.1371/journal.pone.0235514. eCollection 2020. PLoS One. 2020. PMID: 32645031 Free PMC article.
References
-
- Hay SI, et al., Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the global burden of disease study 2016. 2017. The Lancet. 2017;390(10100):1260–1344. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
