

Novel Concepts for Inducing Final Oocyte Maturation in In Vitro Fertilization Treatment
- PMID: 29982525
- PMCID: PMC6173475
- DOI: 10.1210/er.2017-00236
Novel Concepts for Inducing Final Oocyte Maturation in In Vitro Fertilization Treatment
Abstract
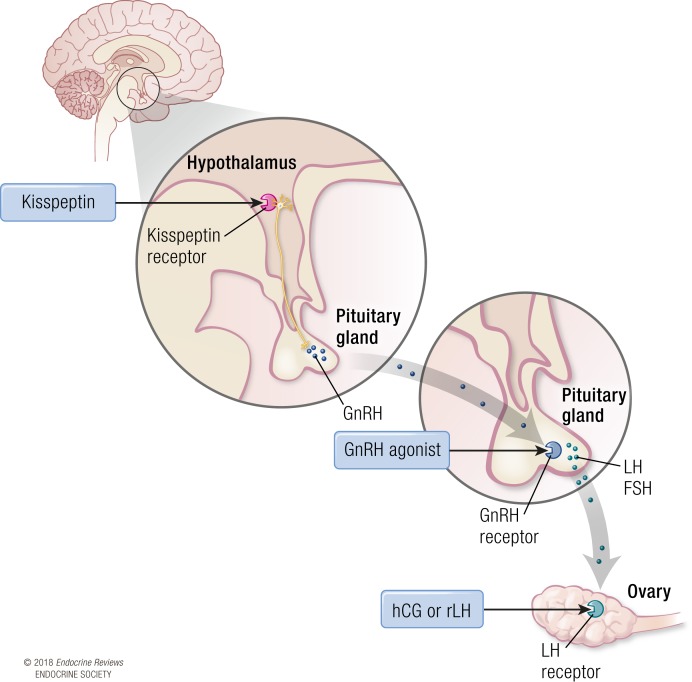
Infertility affects one in six of the population and increasingly couples require treatment with assisted reproductive techniques. In vitro fertilization (IVF) treatment is most commonly conducted using exogenous FSH to induce follicular growth and human chorionic gonadotropin (hCG) to induce final oocyte maturation. However, hCG may cause the potentially life-threatening iatrogenic complication "ovarian hyperstimulation syndrome" (OHSS), which can cause considerable morbidity and, rarely, even mortality in otherwise healthy women. The use of GnRH agonists (GnRHas) has been pioneered during the last two decades to provide a safer option to induce final oocyte maturation. More recently, the neuropeptide kisspeptin, a hypothalamic regulator of GnRH release, has been investigated as a novel inductor of oocyte maturation. The hormonal stimulus used to induce oocyte maturation has a major impact on the success (retrieval of oocytes and chance of implantation) and safety (risk of OHSS) of IVF treatment. This review aims to appraise experimental and clinical data of hormonal approaches used to induce final oocyte maturation by hCG, GnRHa, both GnRHa and hCG administered in combination, recombinant LH, or kisspeptin. We also examine evidence for the timing of administration of the inductor of final oocyte maturation in relationship to parameters of follicular growth and the subsequent interval to oocyte retrieval. In summary, we review data on the efficacy and safety of the major hormonal approaches used to induce final oocyte maturation in clinical practice, as well as some novel approaches that may offer fresh alternatives in future.
Figures
Similar articles
-
The direct and indirect effects of kisspeptin-54 on granulosa lutein cell function.Hum Reprod. 2018 Feb 1;33(2):292-302. doi: 10.1093/humrep/dex357. Hum Reprod. 2018. PMID: 29206944 Clinical Trial.
-
A novel oocyte maturation trigger using 1500 IU of human chorionic gonadotropin plus 450 IU of follicle-stimulating hormone may decrease ovarian hyperstimulation syndrome across all in vitro fertilization stimulation protocols.J Assist Reprod Genet. 2018 Feb;35(2):297-307. doi: 10.1007/s10815-017-1074-4. Epub 2017 Oct 30. J Assist Reprod Genet. 2018. PMID: 29086322 Free PMC article. Clinical Trial.
-
Endocrine Requirements for Oocyte Maturation Following hCG, GnRH Agonist, and Kisspeptin During IVF Treatment.Front Endocrinol (Lausanne). 2020 Oct 6;11:537205. doi: 10.3389/fendo.2020.537205. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33123084 Free PMC article.
-
Gonadotropin-releasing hormone agonist versus HCG for oocyte triggering in antagonist-assisted reproductive technology.Cochrane Database Syst Rev. 2014 Oct 31;2014(10):CD008046. doi: 10.1002/14651858.CD008046.pub4. Cochrane Database Syst Rev. 2014. PMID: 25358904 Free PMC article. Review.
-
Use of kisspeptin to trigger oocyte maturation during in vitro fertilisation (IVF) treatment.Front Endocrinol (Lausanne). 2022 Sep 6;13:972137. doi: 10.3389/fendo.2022.972137. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36147569 Free PMC article. Review.
Cited by
-
Neurotransmitters, neuropeptides and calcium in oocyte maturation and early development.Front Cell Dev Biol. 2022 Sep 23;10:980219. doi: 10.3389/fcell.2022.980219. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 36211465 Free PMC article. Review.
-
The impact of late follicular progesterone level on in vitro fertilization-intracytoplasmic sperm injection outcome: Case-control study.Int J Reprod Biomed. 2020 May 31;18(5):367-374. doi: 10.18502/ijrm.v13i5.7157. eCollection 2020 May. Int J Reprod Biomed. 2020. PMID: 32637865 Free PMC article.
-
Progestin-primed ovarian stimulation for fertility preservation in women with cancer: A comparative study.PLoS One. 2023 Mar 28;18(3):e0280238. doi: 10.1371/journal.pone.0280238. eCollection 2023. PLoS One. 2023. PMID: 36976781 Free PMC article.
-
Female BMI and Body Weight Is Not Associated with Oocyte Yield and Maturation in hCG, Agonist or Dual Trigger Cycles: A Large Observational Study including 5000 Cycles.J Clin Med. 2023 May 1;12(9):3249. doi: 10.3390/jcm12093249. J Clin Med. 2023. PMID: 37176689 Free PMC article.
-
Impact of Serum Human Chorionic Gonadotropin and Luteinizing Hormone Receptor Expression to Oocyte Maturation Rate: A Study of Controlled Ovarian Stimulation.J Hum Reprod Sci. 2020 Jan-Mar;13(1):46-50. doi: 10.4103/jhrs.JHRS_131_19. Epub 2020 Apr 7. J Hum Reprod Sci. 2020. PMID: 32577068 Free PMC article.
References
-
- World Health Organization Prevalence of moderate and severe disability (in millions), by leading health condition associated with disability, and by age and income status of countries Available at: www.who.int/reproductivehealth/topics/infertility/definitions/en/. Accessed on 1 November 2017.
-
- Ebdrup NH, Assens M, Hougaard CO, Pinborg A, Hageman I, Schmidt L; Centers for Disease Control and Prevention, American Society for Reproductive Medicine, Society for Assisted Reproductive Technology . Assisted reproductive technology (ART) treatment in women with schizophrenia or related psychotic disorder: a national cohort study. Eur J Obstet Gynecol Reprod Biol. 2014;177(May):115–120. - PubMed
-
- Humaidan P, Kol S, Papanikolaou EG; Copenhagen GnRH Agonist Triggering Workshop Group . GnRH agonist for triggering of final oocyte maturation: time for a change of practice? Hum Reprod Update. 2011;17(4):510–524. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
