

Genetic deficiency of NOD2 confers resistance to invasive aspergillosis
- PMID: 29980664
- PMCID: PMC6035256
- DOI: 10.1038/s41467-018-04912-3
Genetic deficiency of NOD2 confers resistance to invasive aspergillosis
Abstract
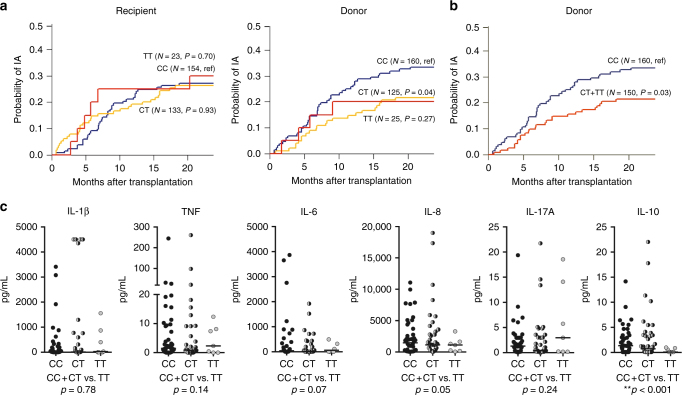
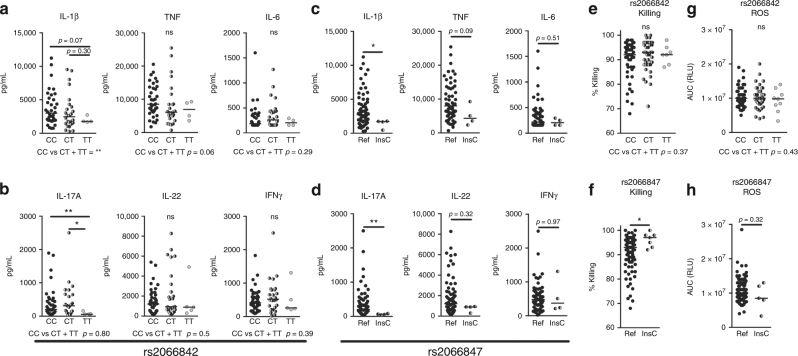
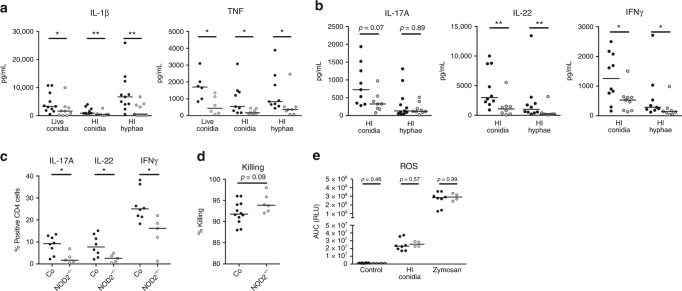
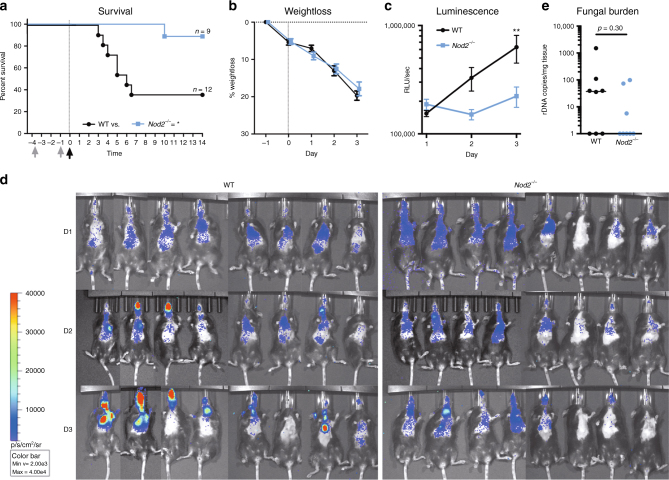
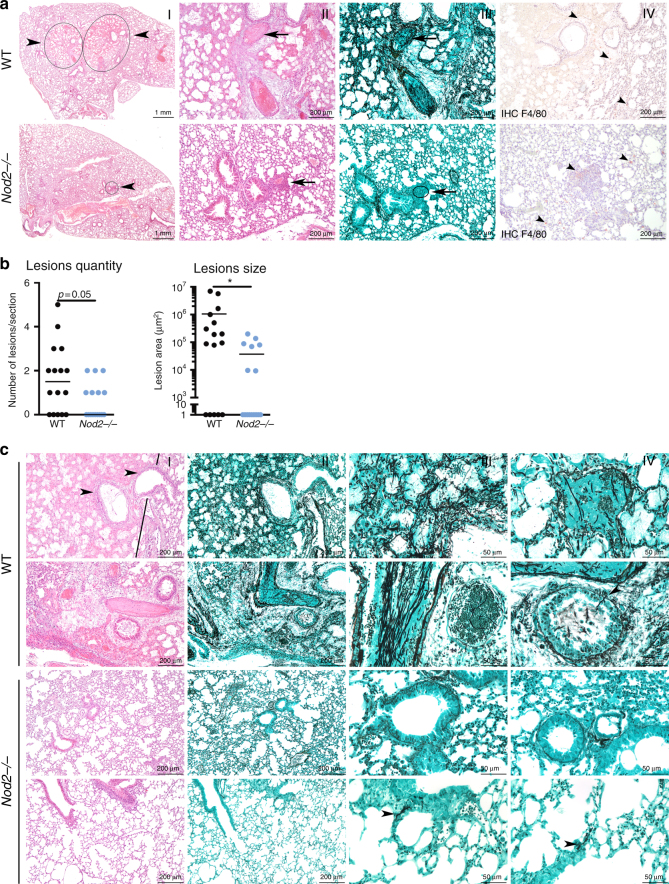
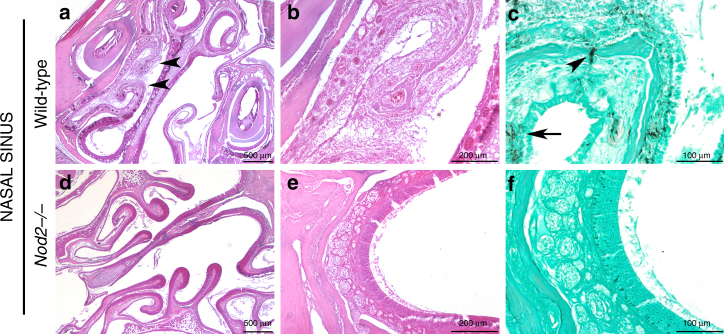
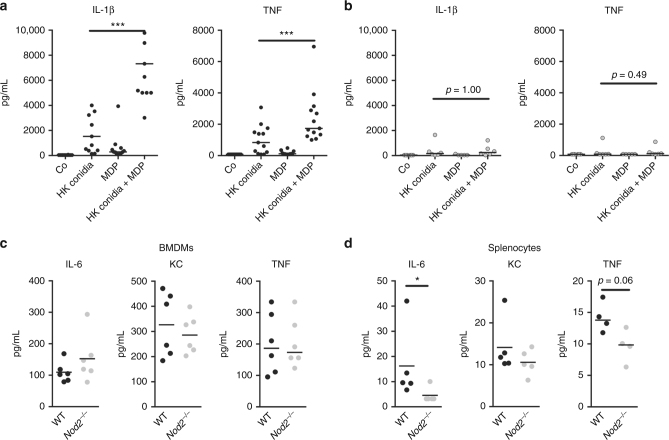
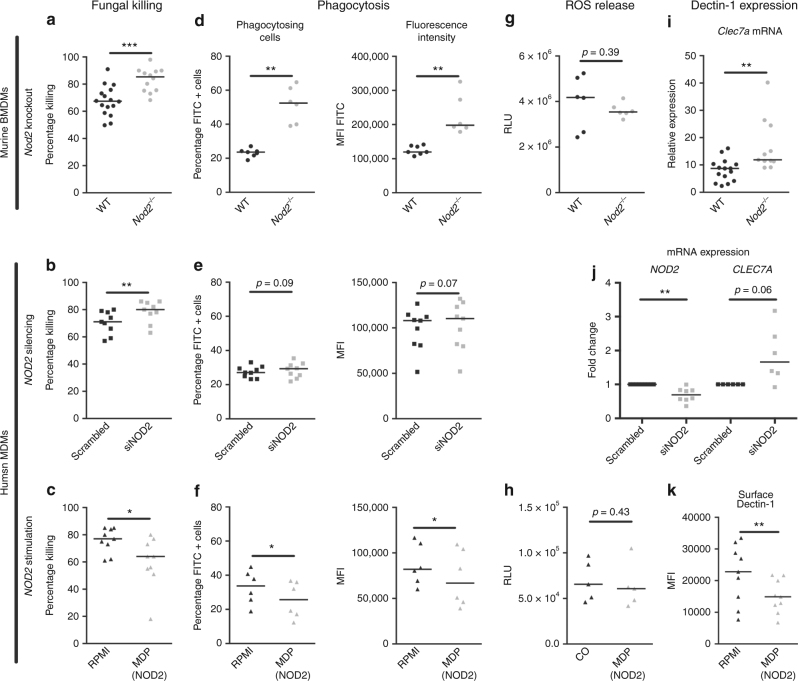
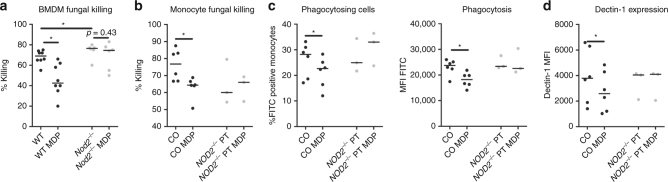
Invasive aspergillosis (IA) is a severe infection that can occur in severely immunocompromised patients. Efficient immune recognition of Aspergillus is crucial to protect against infection, and previous studies suggested a role for NOD2 in this process. However, thorough investigation of the impact of NOD2 on susceptibility to aspergillosis is lacking. Common genetic variations in NOD2 has been associated with Crohn's disease and here we investigated the influence of these genetic variations on the anti-Aspergillus host response. A NOD2 polymorphism reduced the risk of IA after hematopoietic stem-cell transplantation. Mechanistically, absence of NOD2 in monocytes and macrophages increases phagocytosis leading to enhanced fungal killing, conversely, NOD2 activation reduces the antifungal potential of these cells. Crucially, Nod2 deficiency results in resistance to Aspergillus infection in an in vivo model of pulmonary aspergillosis. Collectively, our data demonstrate that genetic deficiency of NOD2 plays a protective role during Aspergillus infection.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Increased susceptibility for aspergillosis and post-transplant immune deficiency in patients with gene variants of TLR4 after stem cell transplantation.Transpl Infect Dis. 2013 Oct;15(5):533-9. doi: 10.1111/tid.12115. Epub 2013 Jul 25. Transpl Infect Dis. 2013. PMID: 23890253
-
Dectin-1 Y238X polymorphism associates with susceptibility to invasive aspergillosis in hematopoietic transplantation through impairment of both recipient- and donor-dependent mechanisms of antifungal immunity.Blood. 2010 Dec 9;116(24):5394-402. doi: 10.1182/blood-2010-04-279307. Epub 2010 Aug 31. Blood. 2010. PMID: 20807886
-
Influence of polymorphisms in innate immunity genes on susceptibility to invasive aspergillosis after stem cell transplantation.PLoS One. 2011 Apr 4;6(4):e18403. doi: 10.1371/journal.pone.0018403. PLoS One. 2011. PMID: 21483748 Free PMC article.
-
Immunogenetics of invasive aspergillosis.Med Mycol. 2011 Apr;49 Suppl 1:S125-36. doi: 10.3109/13693786.2010.516408. Epub 2010 Sep 15. Med Mycol. 2011. PMID: 20840014 Review.
-
Cellular and molecular mechanisms underlying NOD2 risk-associated polymorphisms in Crohn's disease.Immunol Rev. 2014 Jul;260(1):249-60. doi: 10.1111/imr.12193. Immunol Rev. 2014. PMID: 24942694 Review.
Cited by
-
Host immune responses in the central nervous system during fungal infections.Immunol Rev. 2022 Oct;311(1):50-74. doi: 10.1111/imr.13101. Epub 2022 Jun 7. Immunol Rev. 2022. PMID: 35672656 Free PMC article. Review.
-
Effects of Hematopoietic Cell Transplantation on the Pulmonary Immune Response to Infection.Front Pediatr. 2021 Jan 26;9:634566. doi: 10.3389/fped.2021.634566. eCollection 2021. Front Pediatr. 2021. PMID: 33575235 Free PMC article. Review.
-
Challenges and Opportunities in Understanding Genetics of Fungal Diseases: Towards a Functional Genomics Approach.Infect Immun. 2021 Jul 15;89(8):e0000521. doi: 10.1128/IAI.00005-21. Epub 2021 Jul 15. Infect Immun. 2021. PMID: 34031131 Free PMC article. Review.
-
Pathogenicity and virulence of Aspergillus fumigatus.Virulence. 2023 Dec;14(1):2172264. doi: 10.1080/21505594.2023.2172264. Virulence. 2023. PMID: 36752587 Free PMC article. Review.
-
Aspergillus fumigatus and Aspergillosis in 2019.Clin Microbiol Rev. 2019 Nov 13;33(1):e00140-18. doi: 10.1128/CMR.00140-18. Print 2019 Dec 18. Clin Microbiol Rev. 2019. PMID: 31722890 Free PMC article. Review.
References
-
- Ben-Ami R, Lewis RE, Kontoyiannis DP. Enemy of the (immunosuppressed) state: an update on the pathogenesis of Aspergillus fumigatus infection. Br. J. Haematol. 2010;150:406–417. - PubMed
-
- Cunha C, et al. Dectin-1 Y238X polymorphism associates with susceptibility to invasive aspergillosis in hematopoietic transplantation through impairment of both recipient- and donor-dependent mechanisms of antifungal immunity. Blood. 2010;116:5394–5402. doi: 10.1182/blood-2010-04-279307. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
