

The venous ulcer continues to be a clinical challenge: an update
- PMID: 29942813
- PMCID: PMC6003071
- DOI: 10.1186/s41038-018-0119-y
The venous ulcer continues to be a clinical challenge: an update
Abstract
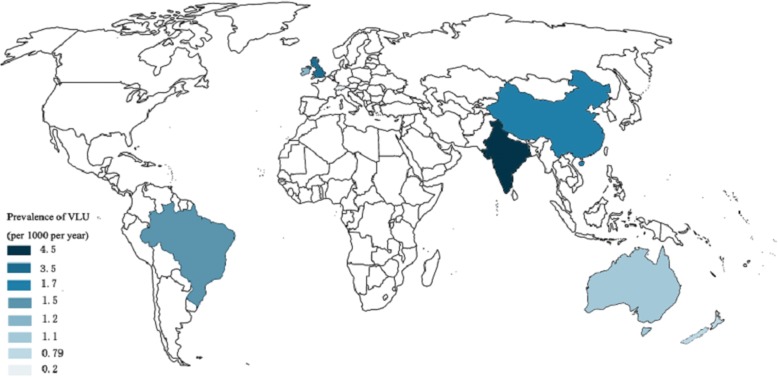
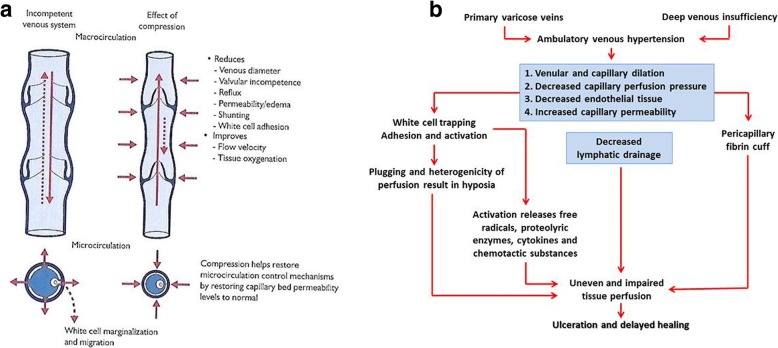
Venous ulcers are a common chronic problem in many countries especially in Northern Europe and USA. The overall prevalence of this condition is 1% rising to 3% in the over 65 years of age. Over the last 25 years, there have been many developments applicable to its diagnosis and treatment. These advances, notwithstanding healing response and recurrence, are variable, and the venous ulcer continues to be a clinical challenge. The pathogenesis of venous ulcers is unrelieved or ambulatory venous hypertension resulting mostly from deep venous thrombosis leading to venous incompetence, lipodermatosclerosis, leucocyte plugging of the capillaries, tissue hypoxia and microvascular dysfunction. It is not known what initiates venous ulcers. Triggers vary from trauma of the lower extremity to scratching to relieve itchy skin over the ankle region. Venous ulcers can be painful, and this condition presents an increasing burden of care. A systematic analysis of the role of technology used for diagnosis and management strongly supports the use of compression as a mainstay of standardised care. It further shows good evidence for the potential of some treatment procedures to accelerate healing. This article reviews the pathogenetic mechanisms, current diagnostic methods and standard care and its limitations.
Keywords: Lipodermatosclerosis; Microcirculatory dysfunction; Technology guidelines; Venous hypertension; Venous ulcer.
Conflict of interest statement
Written informed consent was obtained from the patient for publication of this review and any accompanying images. Acopy of the written consent is available for review by the Editor-in-Chief of this journal.RM has received educational grants from the industry to conduct studies and to present lectures. The other authors declare that they have no competing interests.
Figures

Similar articles
-
Venous Ulcers: Diagnosis and Treatment.Am Fam Physician. 2019 Sep 1;100(5):298-305. Am Fam Physician. 2019. PMID: 31478635 Review.
-
Conservative versus surgical treatment of venous leg ulcers: a prospective, randomized, multicenter trial.J Vasc Surg. 2006 Sep;44(3):563-71. doi: 10.1016/j.jvs.2006.04.053. J Vasc Surg. 2006. PMID: 16950434 Clinical Trial.
-
Diagnosis and treatment of venous ulcers.Am Fam Physician. 2010 Apr 15;81(8):989-96. Am Fam Physician. 2010. PMID: 20387775
-
Risk factors related to the failure of venous leg ulcers to heal with compression treatment.J Vasc Surg. 2009 May;49(5):1242-7. doi: 10.1016/j.jvs.2008.11.069. Epub 2009 Feb 23. J Vasc Surg. 2009. PMID: 19233601 Clinical Trial.
-
Deleterious effects of white cells in the course of skin damage in CVI.Int Angiol. 2002 Jun;21(2 Suppl 1):26-32. Int Angiol. 2002. PMID: 12515977 Review.
Cited by
-
Human Wounds and Its Burden: An Updated Compendium of Estimates.Adv Wound Care (New Rochelle). 2019 Feb 1;8(2):39-48. doi: 10.1089/wound.2019.0946. Epub 2019 Feb 13. Adv Wound Care (New Rochelle). 2019. PMID: 30809421 Free PMC article.
-
In Vitro and In Vivo Evaluation of Bioactive Compounds from Berries for Wound Healing.Curr Dev Nutr. 2024 Jan 14;8(2):102078. doi: 10.1016/j.cdnut.2024.102078. eCollection 2024 Feb. Curr Dev Nutr. 2024. PMID: 38351974 Free PMC article. Review.
-
Tissue regeneration: an overview from stem cells to micrografts.J Int Med Res. 2020 Jun;48(6):300060520914794. doi: 10.1177/0300060520914794. J Int Med Res. 2020. PMID: 32536230 Free PMC article. Review.
-
WoundCareLog APP - A new application to record wound diagnosis and healing.Chin J Traumatol. 2019 Oct;22(5):296-299. doi: 10.1016/j.cjtee.2019.07.003. Epub 2019 Aug 16. Chin J Traumatol. 2019. PMID: 31481277 Free PMC article.
-
Topical Sevoflurane: A Novel Treatment for Chronic Pain Caused by Venous Stasis Ulcers.Anesth Pain Med. 2021 Feb 24;11(1):e112832. doi: 10.5812/aapm.112832. eCollection 2021 Feb. Anesth Pain Med. 2021. PMID: 34221949 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
