

Prevention paradox: Medical students are less inclined to prescribe HIV pre-exposure prophylaxis for patients in highest need
- PMID: 29939488
- PMCID: PMC6016621
- DOI: 10.1002/jia2.25147
Prevention paradox: Medical students are less inclined to prescribe HIV pre-exposure prophylaxis for patients in highest need
Abstract
Introduction: Despite healthcare providers' growing awareness of pre-exposure prophylaxis (PrEP), prescription rates remain low. PrEP is an efficacious HIV prevention strategy recommended for use with condoms but still protective in their absence. Concern about the impact of PrEP on condom use and other risk behaviour is, nonetheless, among the barriers to prescription commonly reported. To understand the implications of this concern for PrEP access, we examined how medical students' willingness to prescribe PrEP varied by patients' condom use and partnering practices. We also assessed the perceived acceptability of various reasons for condom discontinuation with PrEP.
Methods: An online survey was distributed to 854 medical students in the Northeastern US in 2015. Participants (n = 111) were surveyed about their willingness to prescribe PrEP for each of six male patients who systematically differed in their reported condom use (sustained use, sustained nonuse, or discontinuation with PrEP) and partnering practices (single male partner with untreated HIV or multiple male partners of unknown HIV status). Participants also reported perceived acceptability of four reasons for condom discontinuation: pleasure, sexual functioning, intimacy, and conception.
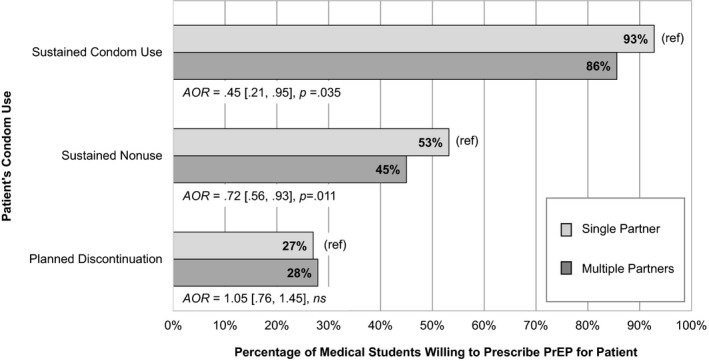
Results: Willingness to prescribe PrEP was inconsistent with patient risk: When the patient used condoms and planned to sustain condom use, most participants were willing to prescribe PrEP - 93% if the patient had a single partner and 86% if the patient had multiple partners. Fewer were willing to prescribe if the patient did not use condoms and planned to sustain nonuse (53% and 45%, respectively) or used condoms but planned to discontinue use (27% and 28%). Significantly fewer participants were willing to prescribe for a patient with multiple partners versus a single partner when the patient reported sustained condom use or sustained condom nonuse. The number of participants who were willing to prescribe was similarly low for a patient with multiple partners versus a single partner when the patient reported that he planned to discontinue condom use. More participants accepted a patient discontinuing condoms for conception (69%) than for intimacy (23%), pleasure (14%), or sexual functioning (13%).
Conclusion: Medical students' clinical judgments were misaligned with patient risk and suggest misconceptions or personal values may undermine provision of optimal HIV prevention services.
Keywords: HIV; health personnel; healthcare disparities; pre-exposure prophylaxis; prescriptions; sexual minorities.
© 2018 The Authors. Journal of the International AIDS Society published by John Wiley & sons Ltd on behalf of the International AIDS Society.
Figures
Similar articles
-
The Role of Social Biases, Race, and Condom Use in Willingness to Prescribe HIV Pre-exposure Prophylaxis to MSM: An Experimental, Vignette-Based Study.J Acquir Immune Defic Syndr. 2022 Dec 1;91(4):353-363. doi: 10.1097/QAI.0000000000003072. Epub 2022 Aug 19. J Acquir Immune Defic Syndr. 2022. PMID: 36288542 Free PMC article.
-
Differences in awareness of and willingness to use pre-exposure prophylaxis and anticipated condom use among serodiscordant couples in Taiwan.AIDS Care. 2018 Oct;30(10):1306-1310. doi: 10.1080/09540121.2018.1481195. Epub 2018 May 30. AIDS Care. 2018. PMID: 29845871
-
Willingness to use PrEP among female university students in Lesotho.PLoS One. 2020 Mar 31;15(3):e0230565. doi: 10.1371/journal.pone.0230565. eCollection 2020. PLoS One. 2020. PMID: 32231394 Free PMC article.
-
Increasing awareness of HIV pre-exposure prophylaxis (PrEP) and willingness to use HIV PrEP among men who have sex with men: a systematic review and meta-analysis of global data.J Int AIDS Soc. 2022 Mar;25(3):e25883. doi: 10.1002/jia2.25883. J Int AIDS Soc. 2022. PMID: 35255193 Free PMC article. Review.
-
[Current status of the female condom in Africa].Sante. 1997 Nov-Dec;7(6):405-15. Sante. 1997. PMID: 9503499 Review. French.
Cited by
-
Behavioral and social science research to support accelerated and equitable implementation of long-acting preexposure prophylaxis.Curr Opin HIV AIDS. 2020 Jan;15(1):66-72. doi: 10.1097/COH.0000000000000596. Curr Opin HIV AIDS. 2020. PMID: 31644482 Free PMC article. Review.
-
Addressing the Sexually Transmitted Infection and HIV Syndemic.JAMA. 2019 Apr 9;321(14):1356-1358. doi: 10.1001/jama.2019.2945. JAMA. 2019. PMID: 30964514 Free PMC article. No abstract available.
-
Socio-Sexual Experiences and Access to Healthcare Among Informal PrEP Users in the Netherlands.AIDS Behav. 2021 Apr;25(4):1236-1246. doi: 10.1007/s10461-020-03085-9. Epub 2020 Nov 16. AIDS Behav. 2021. PMID: 33196938 Free PMC article.
-
Student Education About Pre-exposure Prophylaxis (PrEP) Varies Between Regions of the United States.J Gen Intern Med. 2020 Oct;35(10):2873-2881. doi: 10.1007/s11606-020-05736-y. Epub 2020 Feb 20. J Gen Intern Med. 2020. PMID: 32080792 Free PMC article.
-
Health Care Provider Decisions to Initiate Oral HIV Preexposure Prophylaxis in New York City Public Sexual Health Clinics.Sex Transm Dis. 2023 Jun 1;50(6):386-394. doi: 10.1097/OLQ.0000000000001782. Epub 2023 Feb 8. Sex Transm Dis. 2023. PMID: 36749905 Free PMC article.
References
-
- US Public Health Service . Preexposure prophylaxis for the prevention of HIV infection in the United States – 2017 update: a clinical practice guideline. 2018. [cited 2018 May 10]. Available from: http://www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2017.pdf
-
- Adams LM, Balderson B, Packett BJ II, Brown K, Catz SL. Providers’ perspectives on prescribing pre‐exposure prophylaxis (PrEP) for HIV prevention. HIV Spec. 2015;7:18–25.
-
- Doblecki‐Lewis S, Jones D. Community federally qualified health centers as homes for HIV preexposure prophylaxis: perspectives from South Florida. J Int Assoc Provid AIDS Care. 2016;15:522–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
