

Worldwide burden of cancer attributable to diabetes and high body-mass index: a comparative risk assessment
- PMID: 29803268
- PMCID: PMC5982644
- DOI: 10.1016/S2213-8587(18)30150-5
Worldwide burden of cancer attributable to diabetes and high body-mass index: a comparative risk assessment
Abstract
Background: Diabetes and high body-mass index (BMI) are associated with increased risk of several cancers, and are increasing in prevalence in most countries. We estimated the cancer incidence attributable to diabetes and high BMI as individual risk factors and in combination, by country and sex.
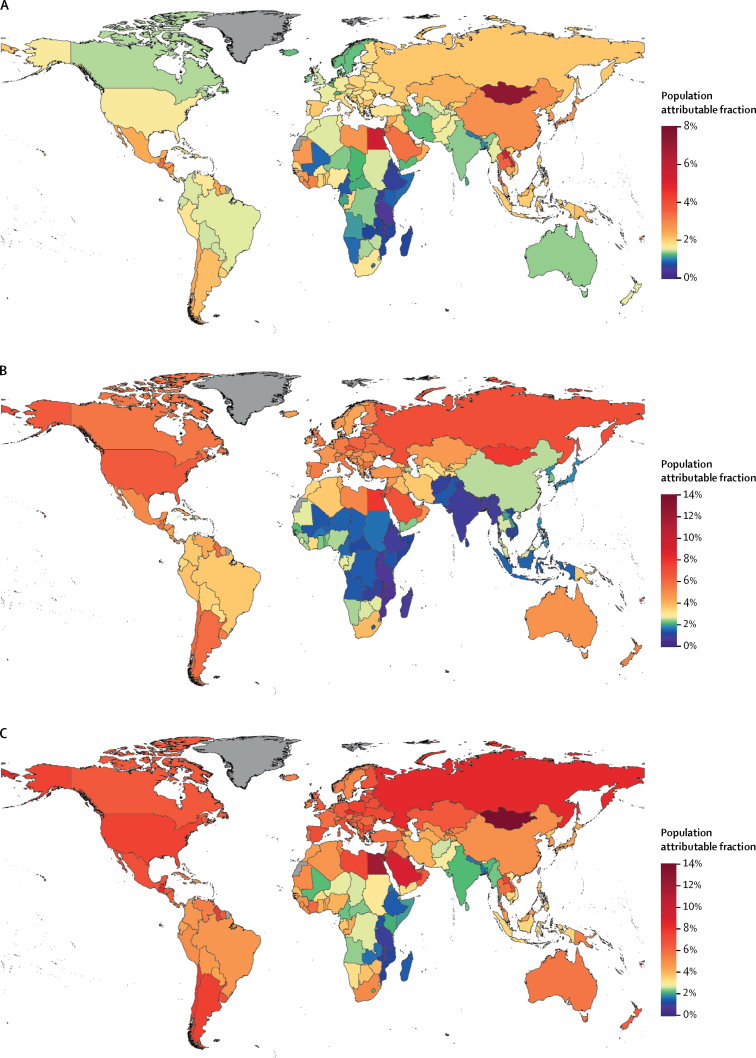
Methods: We estimated population attributable fractions for 12 cancers by age and sex for 175 countries in 2012. We defined high BMI as a BMI greater than or equal to 25 kg/m2. We used comprehensive prevalence estimates of diabetes and BMI categories in 2002, assuming a 10-year lag between exposure to diabetes or high BMI and incidence of cancer, combined with relative risks from published estimates, to quantify contribution of diabetes and high BMI to site-specific cancers, individually and combined as independent risk factors and in a conservative scenario in which we assumed full overlap of risk of diabetes and high BMI. We then used GLOBOCAN cancer incidence data to estimate the number of cancer cases attributable to the two risk factors. We also estimated the number of cancer cases in 2012 that were attributable to increases in the prevalence of diabetes and high BMI from 1980 to 2002. All analyses were done at individual country level and grouped by region for reporting.
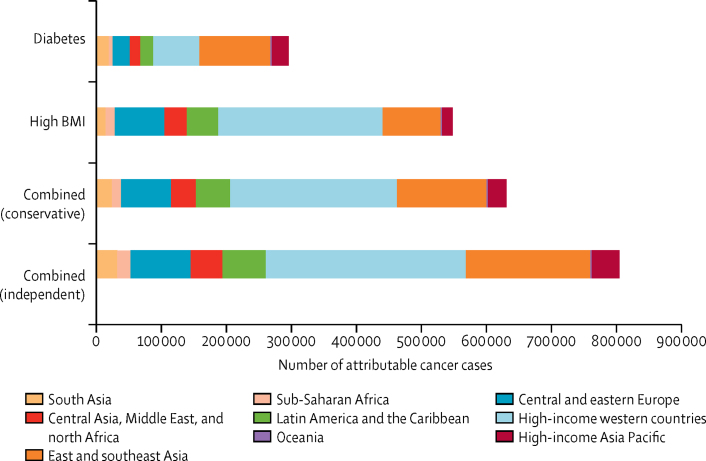
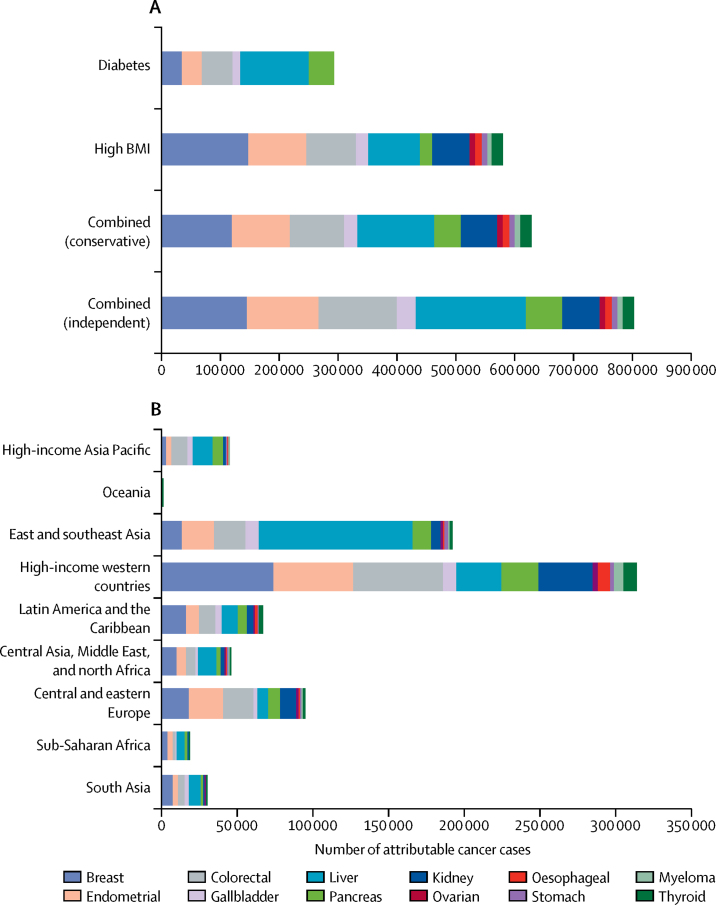
Findings: We estimated that 5·7% of all incident cancers in 2012 were attributable to the combined effects of diabetes and high BMI as independent risk factors, corresponding to 804 100 new cases. 187 600 (24·5%) of 766 000 cases of liver cancer and 121 700 (38·4%) of 317 000 cases of endometrial cancer were attributable to these risk factors. In the conservative scenario, about 4·5% (629 000 new cases) of all incident cancers assessed were attributable to diabetes and high BMI combined. Individually, high BMI (544 300 cases) was responsible for almost twice as many cancer cases as diabetes (293 300 cases). 25·8% of diabetes-related cancers (equating to 75 600 new cases) and 31·9% of high BMI-related cancers (174 040 new cases) were attributable to increases in the prevalence of these risk factors from 1980 to 2002.
Interpretation: A substantial number of cancer cases are attributable to diabetes and high BMI. As the prevalence of these cancer risk factors increases, clinical and public health efforts should focus on identifying optimal preventive and screening measures for whole populations and individual patients.
Funding: NIHR and Wellcome Trust.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Corrected and republished from
-
Worldwide burden of cancer attributable to diabetes and high body-mass index: a comparative risk assessment.Lancet Diabetes Endocrinol. 2018 Feb;6(2):95-104. doi: 10.1016/S2213-8587(17)30366-2. Epub 2017 Nov 28. Lancet Diabetes Endocrinol. 2018. Corrected and republished in: Lancet Diabetes Endocrinol. 2018 Jun;6(6):e6-e15. doi: 10.1016/S2213-8587(18)30150-5 Retraction in: Lancet Diabetes Endocrinol. 2018 Jun;6(6):437. doi: 10.1016/S2213-8587(18)30146-3 PMID: 29195904 Free PMC article. Corrected and republished. Retracted.
Similar articles
-
Worldwide burden of cancer attributable to diabetes and high body-mass index: a comparative risk assessment.Lancet Diabetes Endocrinol. 2018 Feb;6(2):95-104. doi: 10.1016/S2213-8587(17)30366-2. Epub 2017 Nov 28. Lancet Diabetes Endocrinol. 2018. Corrected and republished in: Lancet Diabetes Endocrinol. 2018 Jun;6(6):e6-e15. doi: 10.1016/S2213-8587(18)30150-5 Retraction in: Lancet Diabetes Endocrinol. 2018 Jun;6(6):437. doi: 10.1016/S2213-8587(18)30146-3 PMID: 29195904 Free PMC article. Corrected and republished. Retracted.
-
Global burden of cancer attributable to high body-mass index in 2012: a population-based study.Lancet Oncol. 2015 Jan;16(1):36-46. doi: 10.1016/S1470-2045(14)71123-4. Epub 2014 Nov 26. Lancet Oncol. 2015. PMID: 25467404 Free PMC article.
-
Cancers in France in 2015 attributable to high body mass index.Cancer Epidemiol. 2018 Feb;52:15-19. doi: 10.1016/j.canep.2017.11.006. Epub 2017 Nov 20. Cancer Epidemiol. 2018. PMID: 29161609
-
Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment.Lancet Diabetes Endocrinol. 2014 Aug;2(8):634-47. doi: 10.1016/S2213-8587(14)70102-0. Epub 2014 May 16. Lancet Diabetes Endocrinol. 2014. PMID: 24842598 Free PMC article. Review.
-
Obesity as an Avoidable Cause of Cancer (Attributable Risks).Recent Results Cancer Res. 2016;208:243-256. doi: 10.1007/978-3-319-42542-9_13. Recent Results Cancer Res. 2016. PMID: 27909911 Review.
Cited by
-
Assessing health-related quality of life and clinical outcomes of patients with diabetes accessing healthcare in two public hospitals in south-eastern Ghana: a cross-sectional descriptive study.Qual Life Res. 2024 Apr;33(4):1095-1105. doi: 10.1007/s11136-023-03589-6. Epub 2024 Feb 7. Qual Life Res. 2024. PMID: 38326547
-
Heparanase contributes to pancreatic carcinoma progression through insulin-dependent glucose uptake.Front Cell Dev Biol. 2023 Nov 22;11:1287084. doi: 10.3389/fcell.2023.1287084. eCollection 2023. Front Cell Dev Biol. 2023. PMID: 38078007 Free PMC article.
-
The effect of body acid-base state and manipulations on body glucose regulation in human.Eur J Clin Nutr. 2020 Aug;74(Suppl 1):20-26. doi: 10.1038/s41430-020-0692-6. Eur J Clin Nutr. 2020. PMID: 32873953 Review.
-
Improved preoperative risk stratification with CA-125 in low-grade endometrial cancer: a multicenter prospective cohort study.J Gynecol Oncol. 2019 Sep;30(5):e70. doi: 10.3802/jgo.2019.30.e70. J Gynecol Oncol. 2019. PMID: 31328454 Free PMC article.
-
Global incidence, mortality and temporal trends of cancer in children: A joinpoint regression analysis.Cancer Med. 2023 Jan;12(2):1903-1911. doi: 10.1002/cam4.5009. Epub 2022 Jul 13. Cancer Med. 2023. PMID: 35822443 Free PMC article.
References
-
- NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017 doi: 10.1016/S0140-6736(17)32129-3. published online Oct 10. - DOI - PMC - PubMed
-
- World Cancer Research Fund. American Institute for Cancer Research Food . World Cancer Research Fund; London: 2011. Continuous update project. Colorectal cancer 2011 report. Nutrition, physical activity, and the prevention of colorectal cancer.
-
- World Cancer Research Fund. American Institute for Cancer Research . World Cancer Research; London: 2015. Continuous update project. Diet, nutrition, physical activity and gallbladder cancer.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
