

Alirocumab as add-on therapy to statins: current evidence and clinical potential
- PMID: 29792380
- PMCID: PMC6009079
- DOI: 10.1177/1753944718775352
Alirocumab as add-on therapy to statins: current evidence and clinical potential
Abstract
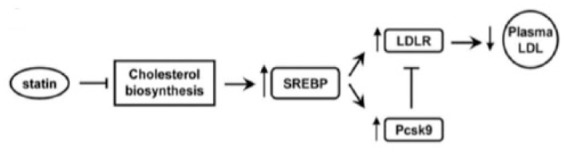
Atherosclerotic cardiovascular diseases (ASCVDs) are associated with a substantial mortality, physical morbidity, and mental disability. Elevated plasma low-density lipoprotein cholesterol (LDL-C) levels play a major role in the pathophysiology of ASCVDs. Statins have been shown to reduce ASCVD risk and associated events and are recommended as first-line therapy for treatment of hypercholesterolemia by current international guidelines. The key issue is to attain guideline-recommended LDL-C levels (below 70 mg/dl) for patients at very high cardiovascular risk. However, many high-risk and very-high-risk patients on statin therapy remain beyond treatment goals despite lifestyle modification and statins, and are exposed to a high risk of future cardiovascular events including myocardial infarction (MI), stroke, revascularization procedures, and death. This clearly emphasizes the urgent need for additional LDL-C reduction with new therapeutic strategies to target these highly atherogenic particles and to further reduce the burden of ASCVDs. Proprotein convertase subtilisin/kexin type 9 (PCSK9) plays a major role as a key regulator of the hepatic LDL receptor recycling process. Developments over the past 15 years have demonstrated PCSK9 inhibition to be a novel therapeutic strategy to manage increased LDL-C levels. A number of clinical studies using humanized monoclonal antibody technology against PCSK9 have shown profound reductions of LDL-C levels when used either alone or in combination with statin therapy. Recently, the first cardiovascular outcome study demonstrated a significant reduction of ASCV events when evolocumab was added to a statin therapy. This review will discuss current knowledge about antibody-mediated PCSK9 inhibition as add-on therapy to statin and the clinical potential that may be expected.
Keywords: alirocumab; cholesterol metabolism; genetics; proprotein convertase subtilisin/kexin type 9 inhibition; statins.
Conflict of interest statement
Figures
Similar articles
-
Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors: Present perspectives and future horizons.Nutr Metab Cardiovasc Dis. 2016 Oct;26(10):853-62. doi: 10.1016/j.numecd.2016.05.006. Epub 2016 May 30. Nutr Metab Cardiovasc Dis. 2016. PMID: 27352986 Review.
-
Alirocumab therapy in individuals with type 2 diabetes mellitus and atherosclerotic cardiovascular disease: analysis of the ODYSSEY DM-DYSLIPIDEMIA and DM-INSULIN studies.Cardiovasc Diabetol. 2019 Nov 9;18(1):149. doi: 10.1186/s12933-019-0951-9. Cardiovasc Diabetol. 2019. PMID: 31706300 Free PMC article.
-
Statin intolerance in heterozygous familial hypercolesterolemia with cardiovascular disease: After PCSK-9 antibodies what else?Eur J Prev Cardiol. 2017 Sep;24(14):1528-1531. doi: 10.1177/2047487317712419. Epub 2017 May 30. Eur J Prev Cardiol. 2017. PMID: 28555526
-
Low Density Lipoprotein (LDL) Cholesterol as a Causal Role for Atherosclerotic Disease: Potential Role of PCSK9 Inhibitors.High Blood Press Cardiovasc Prev. 2019 Jun;26(3):199-207. doi: 10.1007/s40292-019-00323-7. Epub 2019 Jun 24. High Blood Press Cardiovasc Prev. 2019. PMID: 31236902 Review.
-
Residual Inflammatory Risk on Treatment With PCSK9 Inhibition and Statin Therapy.Circulation. 2018 Jul 10;138(2):141-149. doi: 10.1161/CIRCULATIONAHA.118.034645. Epub 2018 May 1. Circulation. 2018. PMID: 29716940 Free PMC article. Clinical Trial.
Cited by
-
Reduction of Cardiovascular Risk Using Proprotein Convertase Subtilisin/Kexin Type 9 Inhibitors in Patients With Acute Coronary Syndrome: A Systematic Review.Cureus. 2023 Feb 5;15(2):e34648. doi: 10.7759/cureus.34648. eCollection 2023 Feb. Cureus. 2023. PMID: 36895542 Free PMC article. Review.
-
Genetics, Safety, Cost-Effectiveness, and Accessibility of Injectable Lipid-Lowering Agents: A Narrative Review.J Lipids. 2023 Mar 8;2023:2025490. doi: 10.1155/2023/2025490. eCollection 2023. J Lipids. 2023. PMID: 36935878 Free PMC article. Review.
-
Systematic analysis of long non-coding RNA and mRNA expression changes in ApoE-deficient mice during atherosclerosis.Mol Cell Biochem. 2019 Dec;462(1-2):61-73. doi: 10.1007/s11010-019-03610-y. Epub 2019 Aug 24. Mol Cell Biochem. 2019. PMID: 31446617 Free PMC article.
References
-
- Stone NJ Robinson JG Lichtenstein AH et al. .;. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63(pt B): 2889–2934. - PubMed
-
- Expert Dyslipidemia Panel of the International Atherosclerosis Society Panel Members. An International Atherosclerosis Society Position Paper: global recommendations for the management of dyslipidemia: full report. J Clin Lipidol 2014; 8: 29–60. - PubMed
-
- Reiner Z, Catapano AL, De Backer G, et al. ESC/EAS guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J 2011; 32: 1769–1818. - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016; 37: 2315–2381. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
