

Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence
- PMID: 29662768
- PMCID: PMC5866399
- DOI: 10.1016/j.jot.2016.11.001
Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence
Abstract
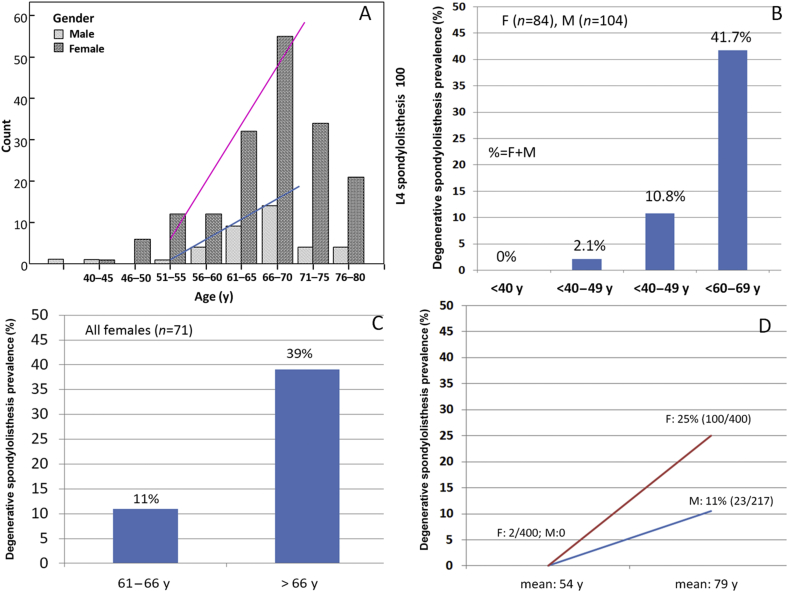
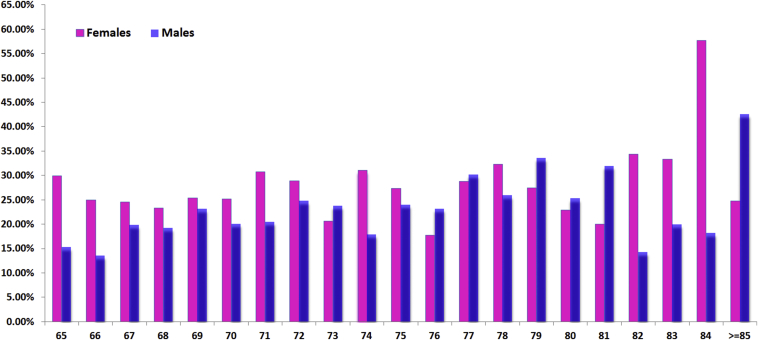
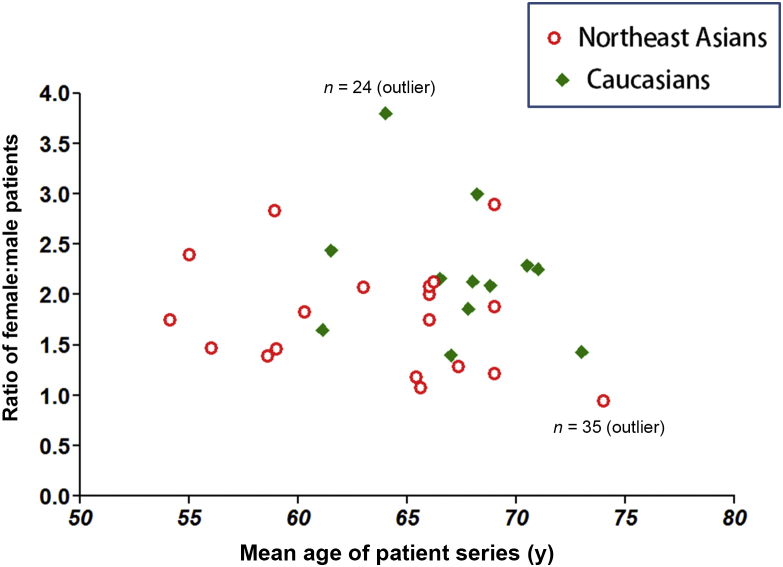
The epidemiology of lumbar degenerative spondylolisthesis (DS) remains controversial. We performed a systematic review with the aim of gaining a better understanding of the prevalence of DS in the general population. The results showed that the prevalence of DS is very gender- and age-specific. Few women and men develop DS before they are 50 years old. After 50 years of age, both women and men begin to develop DS, with women having a faster rate of development than men. For elderly Chinese (≥ 65 years, mean age: 72.5 years), large population-based studies MsOS (Hong Kong, females: n = 2000) and MrOS (Hong Kong, males: n = 2000) showed DS prevalence was 25.0% in women and 19.1% in men. The female:male (F:M) prevalence ratio was 1.3:1. The published data for MsOS (USA) and MrOS (USA) studies seem to show that elderly Caucasian Americans have a higher DS prevalence, being approximately 60-70% higher than elderly Chinese; however, the F:M prevalence ratio was similar to the elderly Chinese population. Patient data showed that female patients more often received surgical treatment than male and preliminary data showed the ratio of female to male patients receiving surgical treatment did not differ between Northeast Asians (Chinese, Japanese, and Korean), Europeans, and American Caucasians, being around 2:1 in the elderly population. The existing data also suggest that menopause may be a contributing factor for the accelerated development of DS in postmenopausal women. The translational potential of this article: A better understanding of epidemiology of lumbar degenerative spondylolisthesis can support patient consultation and treatment planning.
Keywords: Caucasian; Chinese; degenerative spondylolisthesis; men; prevalence; women.
Figures
Similar articles
-
'Healthier Chinese spine': an update of osteoporotic fractures in men (MrOS) and in women (MsOS) Hong Kong spine radiograph studies.Quant Imaging Med Surg. 2022 Mar;12(3):2090-2105. doi: 10.21037/qims-2021-07. Quant Imaging Med Surg. 2022. PMID: 35284274 Free PMC article. Review.
-
Prevalence and risk factors of lumbar spondylolisthesis in elderly Chinese men and women.Eur Radiol. 2014 Feb;24(2):441-8. doi: 10.1007/s00330-013-3041-5. Epub 2013 Oct 15. Eur Radiol. 2014. PMID: 24126641 Free PMC article.
-
Reoperation rate and risk factors of elective spinal surgery for degenerative spondylolisthesis: minimum 5-year follow-up.Spine J. 2015 Jul 1;15(7):1536-44. doi: 10.1016/j.spinee.2015.02.009. Epub 2015 Feb 11. Spine J. 2015. PMID: 25681581
-
Lower Prevalence and Severity of Degenerative Changes in the Lumbar Spine in Elderly Hong Kong Chinese Compared With Age-Matched Italian Caucasian Women.Spine (Phila Pa 1976). 2022 Dec 15;47(24):1710-1718. doi: 10.1097/BRS.0000000000004445. Epub 2022 Aug 4. Spine (Phila Pa 1976). 2022. PMID: 35943213
-
Does Concomitant Degenerative Spondylolisthesis Influence the Outcome of Decompression Alone in Degenerative Lumbar Spinal Stenosis? A Meta-Analysis of Comparative Studies.World Neurosurg. 2019 Mar;123:226-238. doi: 10.1016/j.wneu.2018.11.246. Epub 2018 Dec 18. World Neurosurg. 2019. PMID: 30576810 Review.
Cited by
-
Gut microbiome dysbiosis is associated with lumbar degenerative spondylolisthesis in symptomatic patients.JOR Spine. 2024 Oct 10;7(4):e70005. doi: 10.1002/jsp2.70005. eCollection 2024 Dec. JOR Spine. 2024. PMID: 39398942 Free PMC article.
-
Evaluating the efficacy and suggesting technical optimizations for endoscopic lumbar interbody fusion across different lumbar spondylolisthesis types.Heliyon. 2024 Jun 6;10(11):e32576. doi: 10.1016/j.heliyon.2024.e32576. eCollection 2024 Jun 15. Heliyon. 2024. PMID: 38961964 Free PMC article.
-
A 2-Year Cost Analysis of Maximum Nonoperative Treatments in Patients With Symptomatic Lumbar Stenosis or Spondylolisthesis That Ultimately Required Surgery.Global Spine J. 2019 Jun;9(4):424-433. doi: 10.1177/2192568218824956. Epub 2019 Feb 18. Global Spine J. 2019. PMID: 31218202 Free PMC article.
-
Comparison of (Partial) economic evaluations of transforaminal lumbar interbody fusion (TLIF) versus Posterior lumbar interbody fusion (PLIF) in adults with lumbar spondylolisthesis: A systematic review.PLoS One. 2021 Feb 11;16(2):e0245963. doi: 10.1371/journal.pone.0245963. eCollection 2021. PLoS One. 2021. PMID: 33571291 Free PMC article.
-
The Functional Outcome of Surgical Management of Spondylolisthesis with Posterior Stabilization and Fusion.J Orthop Case Rep. 2024 Jan;14(1):119-124. doi: 10.13107/jocr.2024.v14.i01.4170. J Orthop Case Rep. 2024. PMID: 38292104 Free PMC article.
References
-
- Farfan H.F. The pathological anatomy of degenerative spondylolisthesis. A cadaver study. Spine (Phila Pa 1976) 1980;5(5):412–418. - PubMed
-
- Newman P.H. The etiology of spondylolisthesis. J Bone Joint Surg [Br] 1963;45:39–59.
-
- Hosoe H., Ohmori K. Degenerative lumbosacral spondylolisthesis: possible factors which predispose the fifth lumbar vertebra to slip. J Bone Joint Surg Br. 2008;90(3):356–359. - PubMed
-
- Berlemann U., Jeszenszky D.J., Bühler D.W., Harms J. The role of lumbar lordosis, vertebral end-plate inclination, disc height, and facet orientation in degenerative spondylolisthesis. J Spinal Disord. 1999;12(1):68–73. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
