

Regular Aerobic, Resistance, and Cross-Training Exercise Prevents Reduced Vascular Function Following a High Sugar or High Fat Mixed Meal in Young Healthy Adults
- PMID: 29568273
- PMCID: PMC5853082
- DOI: 10.3389/fphys.2018.00183
Regular Aerobic, Resistance, and Cross-Training Exercise Prevents Reduced Vascular Function Following a High Sugar or High Fat Mixed Meal in Young Healthy Adults
Abstract
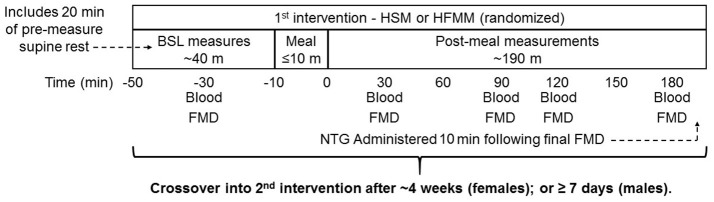
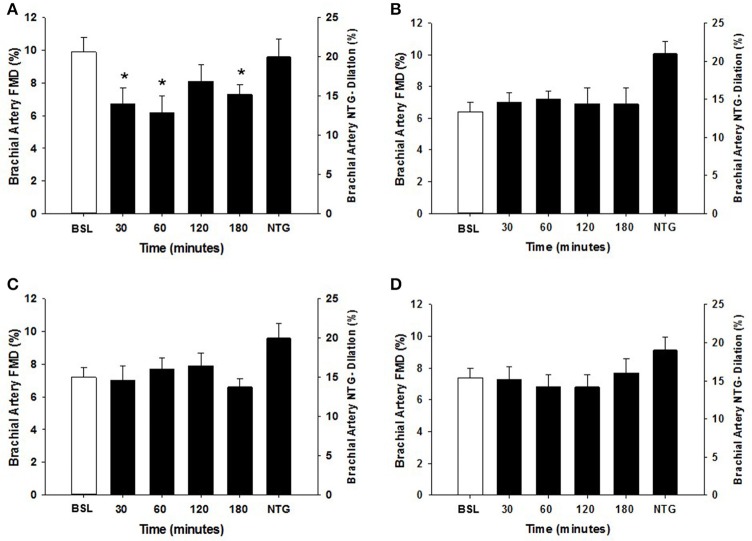
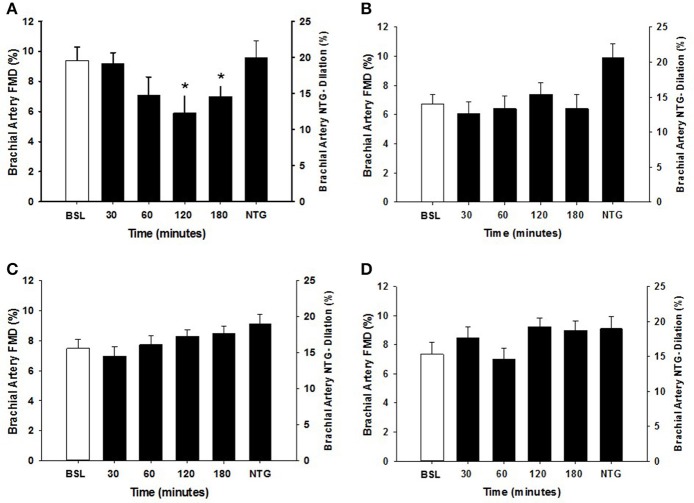
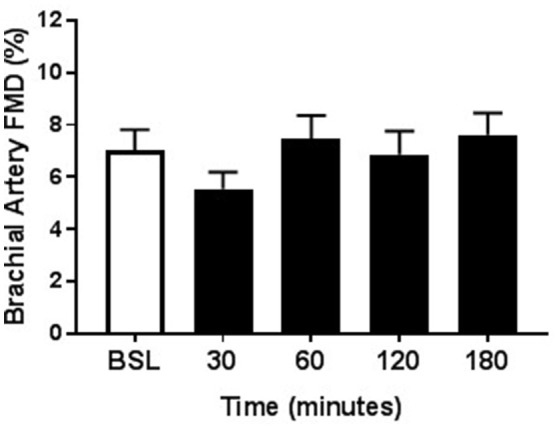
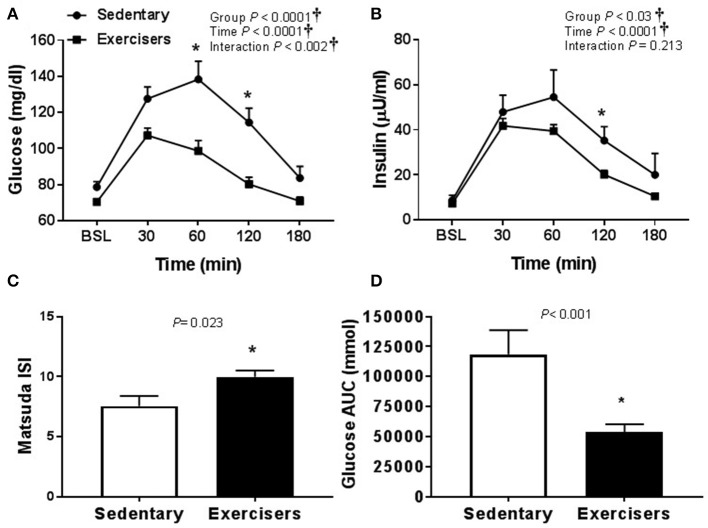
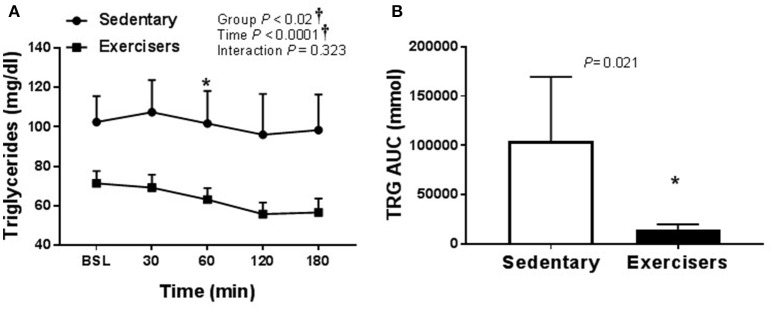
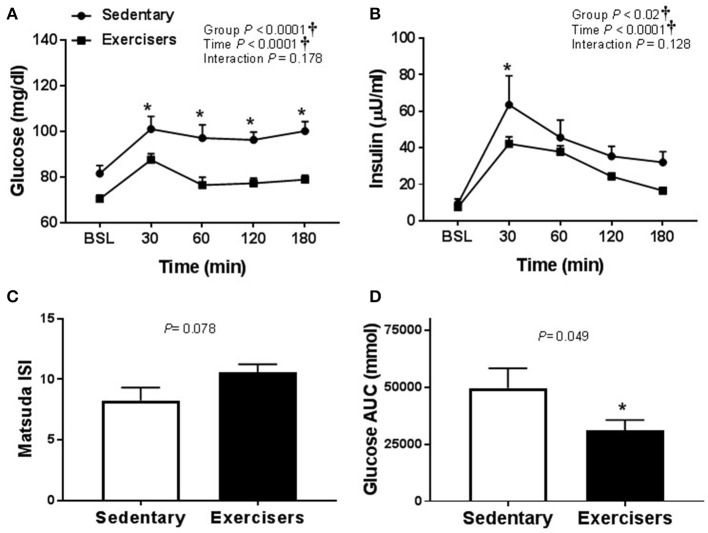
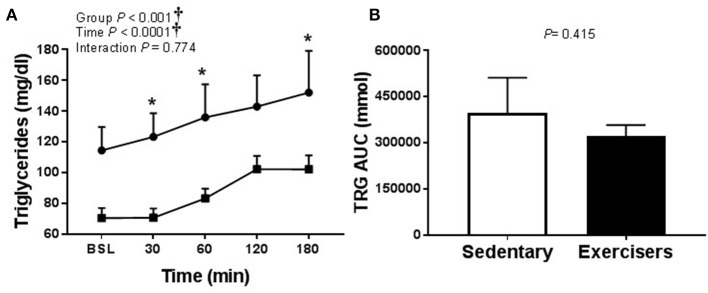
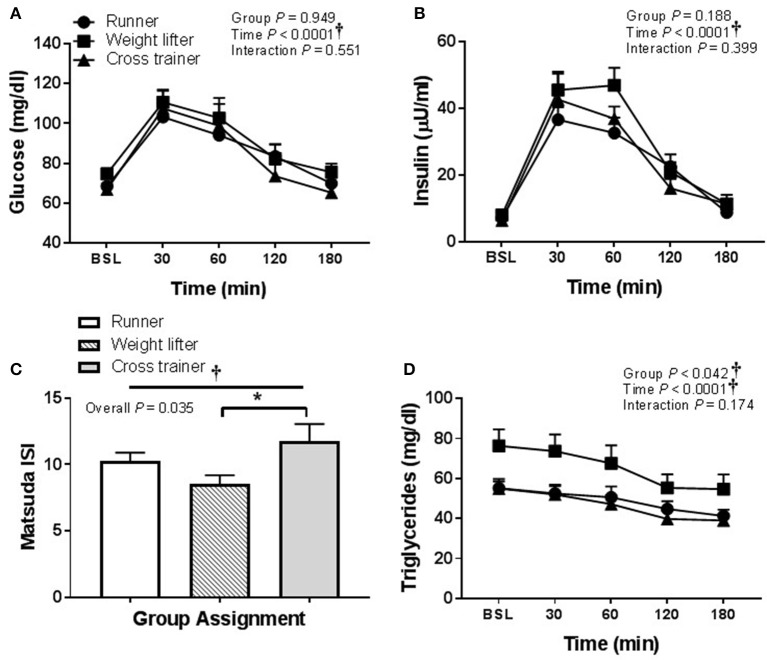
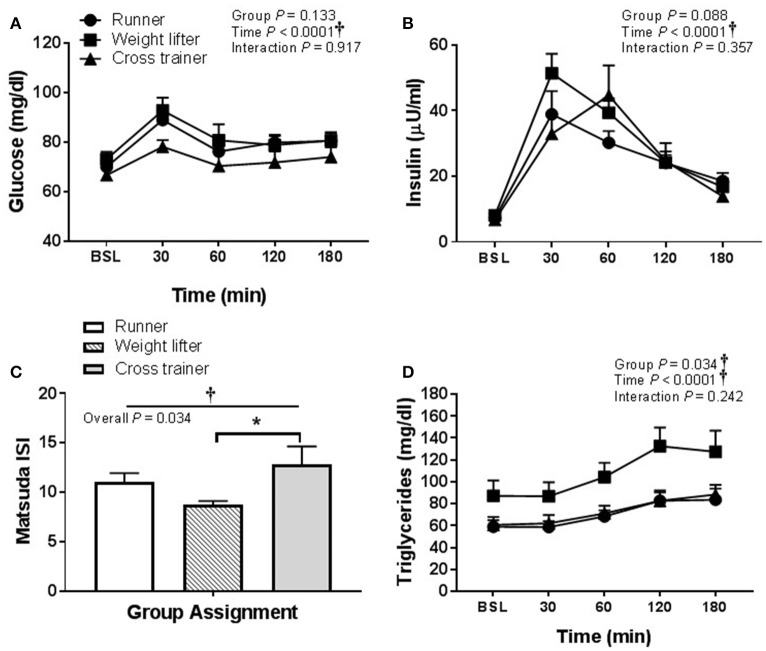
The postprandial state can negatively influence flow mediated dilation (FMD), a predictor of atherosclerosis and cardiovascular disease. This investigation was designed to determine the effect of regular aerobic and/or resistance exercise on postprandial FMD after a high sugar or high fat mixed meal. Forty-five healthy participants were recruited from one of four groups: lean sedentary (SED), runners, weight lifters, and cross-trainers. Participants were randomly crossed over to a high sugar meal (HSM) and a high fat mixed meal (HFMM; both fat and carbohydrate). Pre-and postprandial endothelial function was assessed for both meals using brachial artery FMD. Plasma lipids, insulin, glucose, hs-CRP, and SOD were also measured with both meals. Endothelium-independent dilation was determined via sublingual nitroglycerin. Brachial artery FMD was reduced in SED following the HSM (9.9 ± 0.9% at baseline, peak reduction at 60 min 6.5 ± 1.0%) and the HFMM (9.4 ± 0.9% at baseline, peak reduction at 120 min 5.9 ± 1.2%; P < 0.05 for both, Mean ± SEM). There was no change in FMD after either HSM or HFMM in runners, weight lifters, and cross-trainers. Post-prandial increases in blood glucose, insulin and triglycerides were less pronounced in the exercisers compared to SED. In addition, exercisers presented lower baseline plasma hs-CRP and higher SOD activity. Nitroglycerin responses were similar among groups. These results suggest that endothelial function is reduced in sedentary adults after a HSM or HFMM, but not in regular aerobic or resistance exercisers. This response may be due to favorable postprandial metabolic responses or lower postprandial levels of inflammation and oxidative stress. These findings may help to explain the cardioprotective effect of exercise.
Keywords: arteriosclerosis; dietary carbohydrates; dietary fats; endothelium; postprandial lipemia; regular exercise; vascular; vasodilation.
Figures
Similar articles
-
Resistance and aerobic exercise protects against acute endothelial impairment induced by a single exposure to hypertension during exertion.J Appl Physiol (1985). 2011 Apr;110(4):1013-20. doi: 10.1152/japplphysiol.00438.2010. Epub 2011 Jan 20. J Appl Physiol (1985). 2011. PMID: 21252216 Free PMC article.
-
Acute Peanut Consumption Alters Postprandial Lipids and Vascular Responses in Healthy Overweight or Obese Men.J Nutr. 2017 May;147(5):835-840. doi: 10.3945/jn.116.246785. Epub 2017 Mar 29. J Nutr. 2017. PMID: 28356431 Free PMC article. Clinical Trial.
-
High-intensity interval exercise attenuates but does not eliminate endothelial dysfunction after a fast food meal.Am J Physiol Heart Circ Physiol. 2018 Feb 1;314(2):H188-H194. doi: 10.1152/ajpheart.00384.2017. Epub 2017 Nov 3. Am J Physiol Heart Circ Physiol. 2018. PMID: 29101171 Clinical Trial.
-
The effect of acute exercise on endothelial function following a high-fat meal.Eur J Appl Physiol. 2006 Oct;98(3):256-62. doi: 10.1007/s00421-006-0272-z. Epub 2006 Aug 3. Eur J Appl Physiol. 2006. PMID: 16896723
-
A Systematic Review of the Impact of Fat Quantity and Fatty Acid Composition on Postprandial Vascular Function in Healthy Adults and Patients at Risk of Cardiovascular Disease.Curr Dev Nutr. 2023 Oct 30;7(12):102025. doi: 10.1016/j.cdnut.2023.102025. eCollection 2023 Dec. Curr Dev Nutr. 2023. PMID: 38076399 Free PMC article. Review.
Cited by
-
Partial Synthetic PPARƳ Derivative Ameliorates Aorta Injury in Experimental Diabetic Rats Mediated by Activation of miR-126-5p Pi3k/AKT/PDK 1/mTOR Expression.Pharmaceuticals (Basel). 2022 Sep 22;15(10):1175. doi: 10.3390/ph15101175. Pharmaceuticals (Basel). 2022. PMID: 36297290 Free PMC article.
-
Mechanisms of Atherosclerosis Induced by Postprandial Lipemia.Front Cardiovasc Med. 2021 Apr 29;8:636947. doi: 10.3389/fcvm.2021.636947. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33996937 Free PMC article. Review.
-
Decreased GlycA after lifestyle intervention among obese, prediabetic adolescent Latinos.J Clin Lipidol. 2019 Jan-Feb;13(1):186-193. doi: 10.1016/j.jacl.2018.09.011. Epub 2018 Sep 22. J Clin Lipidol. 2019. PMID: 30342918 Free PMC article.
-
Device-guided slow breathing alters postprandial oxidative stress in young adult males: A randomized sham-controlled crossover trial.Nutr Metab Cardiovasc Dis. 2023 Jan;33(1):203-209. doi: 10.1016/j.numecd.2022.10.002. Epub 2022 Oct 10. Nutr Metab Cardiovasc Dis. 2023. PMID: 36344308 Free PMC article. Clinical Trial.
-
β-cell dynamics in type 2 diabetes and in dietary and exercise interventions.J Mol Cell Biol. 2022 Nov 30;14(7):mjac046. doi: 10.1093/jmcb/mjac046. J Mol Cell Biol. 2022. PMID: 35929791 Free PMC article. Review.
References
-
- Arena R., Guazzi M., Lianov L., Whitsel L., Berra K., Lavie C. J., et al. . (2015). Healthy lifestyle interventions to combat noncommunicable disease-a novel nonhierarchical connectivity model for key stakeholders: a policy statement from the American Heart Association, European Society of Cardiology, European Association for Cardiovascular Prevention and Rehabilitation, and American College of Preventive Medicine. Eur. Heart J. 36, 2097–2109. 10.1093/eurheartj/ehv207 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous