

Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease. What We Know and Can Do for Our Patients
- PMID: 29554438
- PMCID: PMC6058991
- DOI: 10.1164/rccm.201710-2140CI
Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease. What We Know and Can Do for Our Patients
Erratum in
-
Erratum: Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease: What We Know and Can Do for Our Patients.Am J Respir Crit Care Med. 2018 Sep 15;198(6):824-825. doi: 10.1164/rccm.v198erratum3. Am J Respir Crit Care Med. 2018. PMID: 30907108 Free PMC article. No abstract available.
Abstract
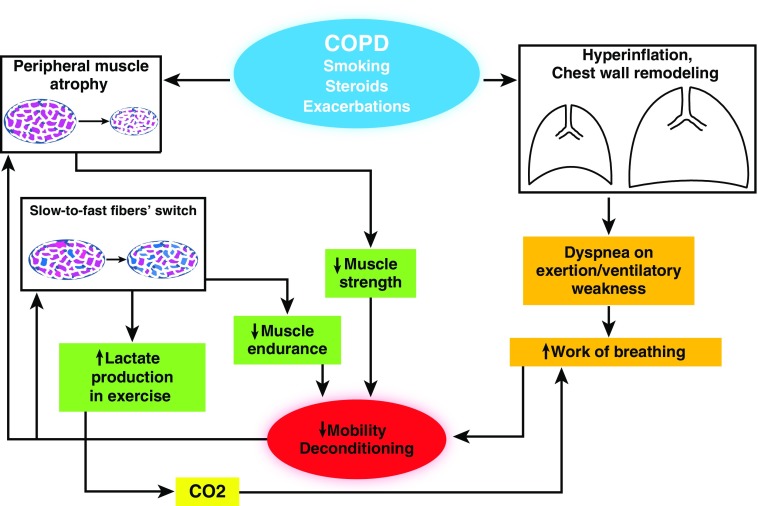
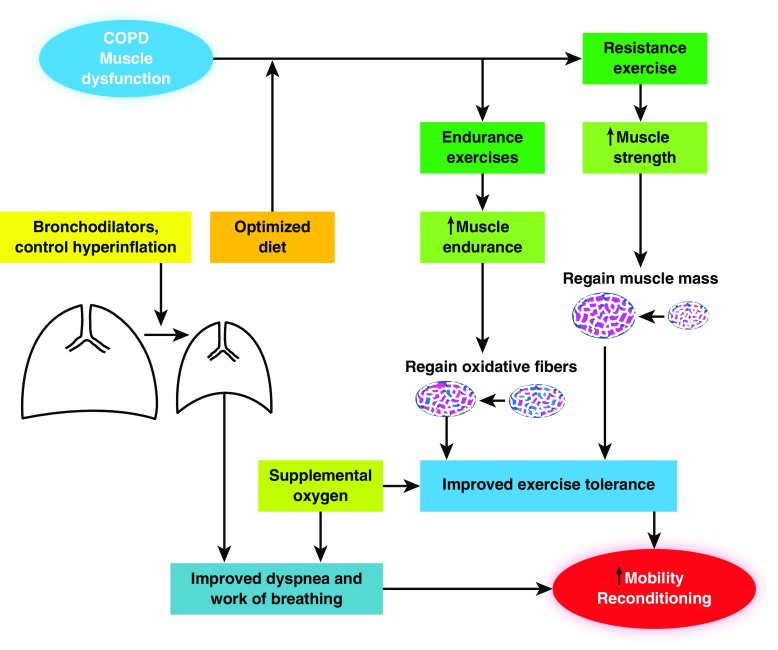
Skeletal muscle dysfunction occurs in patients with chronic obstructive pulmonary disease (COPD) and affects both ventilatory and nonventilatory muscle groups. It represents a very important comorbidity that is associated with poor quality of life and reduced survival. It results from a complex combination of functional, metabolic, and anatomical alterations leading to suboptimal muscle work. Muscle atrophy, altered fiber type and metabolism, and chest wall remodeling, in the case of the respiratory muscles, are relevant etiological contributors to this process. Muscle dysfunction worsens during COPD exacerbations, rendering patients progressively less able to perform activities of daily living, and it is also associated with poor outcomes. Muscle recovery measures consisting of a combination of pulmonary rehabilitation, optimized nutrition, and other strategies are associated with better prognosis when administered in stable patients as well as after exacerbations. A deeper understanding of this process' pathophysiology and clinical relevance will facilitate the use of measures to alleviate its effects and potentially improve patients' outcomes. In this review, a general overview of skeletal muscle dysfunction in COPD is offered to highlight its relevance and magnitude to expert practitioners and scientists as well as to the average clinician dealing with patients with chronic respiratory diseases.
Keywords: chronic obstructive pulmonary disease; fiber switch; muscle wasting; skeletal muscle dysfunction; ventilatory muscles.
Figures
Similar articles
-
The role of MicroRNAs in COPD muscle dysfunction and mass loss: implications on the clinic.Expert Rev Respir Med. 2016 Sep;10(9):1011-22. doi: 10.1080/17476348.2016.1206819. Epub 2016 Jul 14. Expert Rev Respir Med. 2016. PMID: 27348064 Review.
-
Skeletal muscle response to inflammation--lessons for chronic obstructive pulmonary disease.Crit Care Med. 2009 Oct;37(10 Suppl):S372-83. doi: 10.1097/CCM.0b013e3181b6ea1d. Crit Care Med. 2009. PMID: 20046123 Review.
-
Skeletal muscle dysfunction in patients with chronic obstructive pulmonary disease.Int J Chron Obstruct Pulmon Dis. 2008;3(4):637-58. doi: 10.2147/copd.s4480. Int J Chron Obstruct Pulmon Dis. 2008. PMID: 19281080 Free PMC article. Review.
-
Pathophysiology of muscle dysfunction in COPD.J Appl Physiol (1985). 2013 May;114(9):1222-34. doi: 10.1152/japplphysiol.00981.2012. Epub 2013 Mar 21. J Appl Physiol (1985). 2013. PMID: 23519228 Review.
-
[Peripheral muscle dysfunction in chronic obstructive pulmonary disease].Rev Mal Respir. 2002 Sep;19(4):444-53. Rev Mal Respir. 2002. PMID: 12417861 Review. French.
Cited by
-
Diagnostic and clinical values of non-cardiac ultrasound in COPD: A systematic review.BMJ Open Respir Res. 2020 Sep;7(1):e000717. doi: 10.1136/bmjresp-2020-000717. BMJ Open Respir Res. 2020. PMID: 32978244 Free PMC article.
-
Role of Nrf2 and exercise in alleviating COPD-induced skeletal muscle dysfunction.Ther Adv Respir Dis. 2023 Jan-Dec;17:17534666231208633. doi: 10.1177/17534666231208633. Ther Adv Respir Dis. 2023. PMID: 37966017 Free PMC article. Review.
-
Myostatin is involved in skeletal muscle dysfunction in chronic obstructive pulmonary disease via Drp-1 mediated abnormal mitochondrial division.Ann Transl Med. 2022 Feb;10(4):162. doi: 10.21037/atm-22-377. Ann Transl Med. 2022. PMID: 35280400 Free PMC article.
-
Muscle-Bone Crosstalk in Chronic Obstructive Pulmonary Disease.Front Endocrinol (Lausanne). 2021 Sep 28;12:724911. doi: 10.3389/fendo.2021.724911. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34650518 Free PMC article. Review.
-
Locomotor Muscles in COPD: The Rationale for Rehabilitative Exercise Training.Front Physiol. 2020 Jan 14;10:1590. doi: 10.3389/fphys.2019.01590. eCollection 2019. Front Physiol. 2020. PMID: 31992992 Free PMC article. Review.
References
-
- Marquis K, Debigaré R, Lacasse Y, LeBlanc P, Jobin J, Carrier G, et al. Midthigh muscle cross-sectional area is a better predictor of mortality than body mass index in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166:809–813. - PubMed
-
- Shrikrishna D, Patel M, Tanner RJ, Seymour JM, Connolly BA, Puthucheary ZA, et al. Quadriceps wasting and physical inactivity in patients with COPD. Eur Respir J. 2012;40:1115–1122. - PubMed
-
- Vanfleteren LE, Spruit MA, Groenen M, Gaffron S, van Empel VP, Bruijnzeel PL, et al. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187:728–735. - PubMed
-
- Filley GF, Beckwitt HJ, Reeves JT, Mitchell RS. Chronic obstructive bronchopulmonary disease. II. Oxygen transport in two clinical types. Am J Med. 1968;44:26–38. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
