

Opportunities and challenges for human papillomavirus vaccination in cancer
- PMID: 29497146
- PMCID: PMC6454884
- DOI: 10.1038/nrc.2018.13
Opportunities and challenges for human papillomavirus vaccination in cancer
Abstract
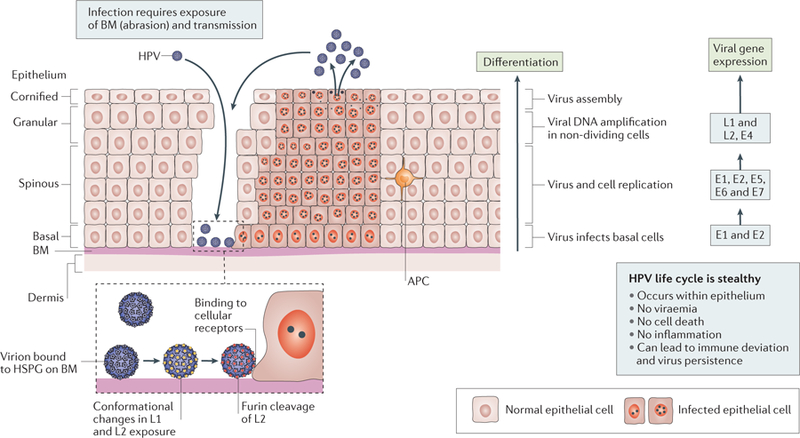
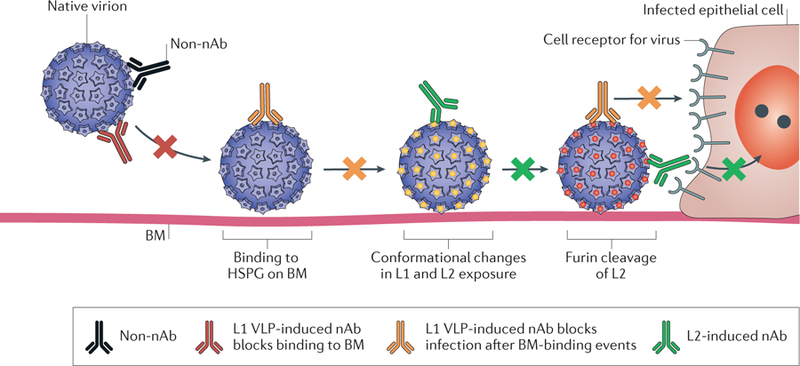
The discovery of genotype 16 as the prototype oncogenic human papillomavirus (HPV) initiated a quarter century of laboratory and epidemiological studies that demonstrated their necessary, but not sufficient, aetiological role in cervical and several other anogenital and oropharyngeal cancers. Early virus-induced immune deviation can lead to persistent subclinical infection that brings the risk of progression to cancer. Effective secondary prevention of cervical cancer through cytological and/or HPV screening depends on regular and widespread use in the general population, but coverage is inadequate in low-resource settings. The discovery that the major capsid antigen L1 could self-assemble into empty virus-like particles (VLPs) that are both highly immunogenic and protective led to the licensure of several prophylactic VLP-based HPV vaccines for the prevention of cervical cancer. The implementation of vaccination programmes in adolescent females is underway in many countries, but their impact critically depends on the population coverage and is improved by herd immunity. This Review considers how our expanding knowledge of the virology and immunology of HPV infection can be exploited to improve vaccine technologies and delivery of such preventive strategies to maximize reductions in HPV-associated disease, including incorporation of an HPV vaccine covering oncogenic types within a standard multitarget paediatric vaccine.
Conflict of interest statement
Competing interests
The authors declare competing interests: see Web version for details.
Figures
Similar articles
-
Quadrivalent Human Papillomavirus Vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP).MMWR Recomm Rep. 2007 Mar 23;56(RR-2):1-24. MMWR Recomm Rep. 2007. PMID: 17380109
-
Developments in L2-based human papillomavirus (HPV) vaccines.Virus Res. 2017 Mar 2;231:166-175. doi: 10.1016/j.virusres.2016.11.020. Epub 2016 Nov 23. Virus Res. 2017. PMID: 27889616 Free PMC article. Review.
-
AS04-adjuvanted human papillomavirus (HPV) types 16 and 18 vaccine (Cervarix®): a review of its use in the prevention of premalignant cervical lesions and cervical cancer causally related to certain oncogenic HPV types.Drugs. 2011 Mar 5;71(4):465-88. doi: 10.2165/11206820-000000000-00000. Drugs. 2011. PMID: 21395359 Review.
-
Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: updated systematic review and meta-analysis.Lancet. 2019 Aug 10;394(10197):497-509. doi: 10.1016/S0140-6736(19)30298-3. Epub 2019 Jun 26. Lancet. 2019. PMID: 31255301 Free PMC article.
-
[Human papillomavirus prophylactic vaccines: stakes and perspectives].Gynecol Obstet Fertil. 2006 Jul-Aug;34(7-8):647-55. doi: 10.1016/j.gyobfe.2006.05.008. Epub 2006 Jun 27. Gynecol Obstet Fertil. 2006. PMID: 16807045 Review. French.
Cited by
-
Unraveling Emerging Anal Cancer Clinical Biomarkers from Current Immuno-Oncogenomics Advances.Mol Diagn Ther. 2024 Mar;28(2):201-214. doi: 10.1007/s40291-023-00692-9. Epub 2024 Jan 24. Mol Diagn Ther. 2024. PMID: 38267771 Free PMC article. Review.
-
Cervical cancer heterogeneity: a constant battle against viruses and drugs.Biomark Res. 2022 Nov 17;10(1):85. doi: 10.1186/s40364-022-00428-7. Biomark Res. 2022. PMID: 36397138 Free PMC article. Review.
-
Lipid Nanoparticles for mRNA Delivery to Enhance Cancer Immunotherapy.Molecules. 2022 Aug 31;27(17):5607. doi: 10.3390/molecules27175607. Molecules. 2022. PMID: 36080373 Free PMC article. Review.
-
Comprehensive Assessment of the Antigenic Impact of Human Papillomavirus Lineage Variation on Recognition by Neutralizing Monoclonal Antibodies Raised against Lineage A Major Capsid Proteins of Vaccine-Related Genotypes.J Virol. 2020 Nov 23;94(24):e01236-20. doi: 10.1128/JVI.01236-20. Print 2020 Nov 23. J Virol. 2020. PMID: 32967963 Free PMC article.
-
A novel C-terminal modification method enhanced the yield of human papillomavirus L1 or chimeric L1-L2 virus-like particles in the baculovirus system.Front Bioeng Biotechnol. 2023 Jan 5;10:1073892. doi: 10.3389/fbioe.2022.1073892. eCollection 2022. Front Bioeng Biotechnol. 2023. PMID: 36686228 Free PMC article.
References
-
-
Forman D et al. Global burden of human papillomavirus and related diseases. Vaccine 30 (Suppl. 5), F12–F23 (2012).
This study provides a recent summary of the global impact of HPV on cancer.
-
-
- Plummer M et al. Global burden of cancers attributable to infections in 2012: a synthetic analysis. Lancet Glob. Health 4, e609–e616 (2016). - PubMed
-
- McCredie MR et al. Natural history of cervical neoplasia and risk of invasive cancer in women with cervical intraepithelial neoplasia 3: a retrospective cohort study. Lancet Oncol 9, 425–434 (2008). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
