

Inhibiting Cellular Senescence: A New Therapeutic Paradigm for Age-Related Osteoporosis
- PMID: 29425296
- PMCID: PMC6276719
- DOI: 10.1210/jc.2017-02694
Inhibiting Cellular Senescence: A New Therapeutic Paradigm for Age-Related Osteoporosis
Abstract
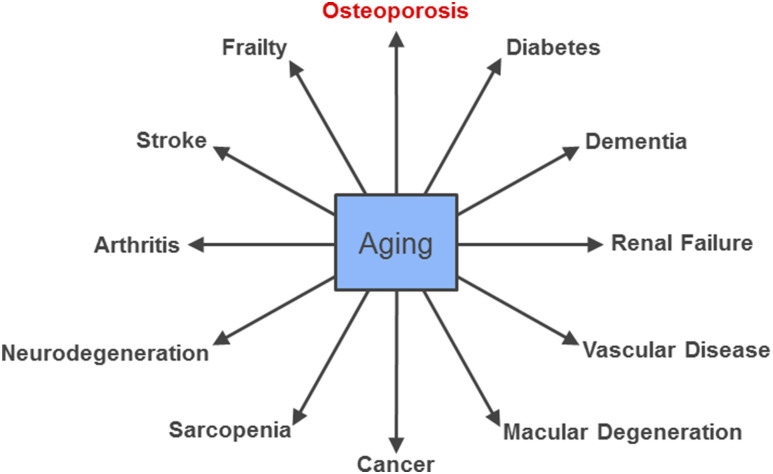
Context: With the aging of the population and projected increase in osteoporotic fractures coupled with the declining use of osteoporosis medications, there is a compelling need for new approaches to treat osteoporosis. Given that age-related osteoporosis generally coexists with multiple other comorbidities (e.g., atherosclerosis, diabetes, frailty) that share aging as the leading risk factor, there is growing interest in the "Geroscience Hypothesis," which posits that manipulation of fundamental aging mechanisms will delay the appearance or severity of multiple chronic diseases because these diseases share aging as the underlying risk factor. In this context, one fundamental aging mechanism that has received considerable attention recently as contributing to multiple age-related morbidities is cellular senescence. This mini-review provides an overview on cellular senescence with a focus on its role in mediating age-related bone loss.
Methods: This summary is based on the authors' knowledge of the field supplemented by a PubMed search using the terms "senescence," "aging," and "bone."
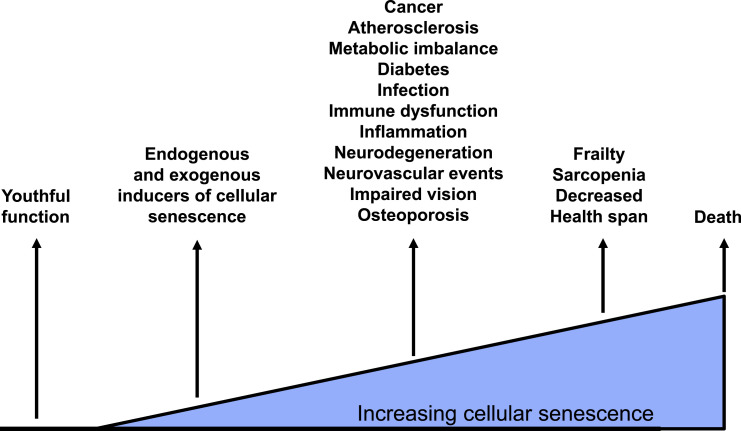
Results: There is compelling evidence from preclinical models and supportive human data demonstrating an increase in senescent cells in the bone microenvironment with aging. These cells produce a proinflammatory secretome that leads to increased bone resorption and decreased bone formation, and approaches that either eliminate senescent cells or impair the production of their proinflammatory secretome have been shown to prevent age-related bone loss in mice.
Conclusions: Targeting cellular senescence represents a novel therapeutic strategy to prevent not only bone loss but potentially multiple age-related diseases simultaneously.
Figures


Similar articles
-
Targeting cellular senescence prevents age-related bone loss in mice.Nat Med. 2017 Sep;23(9):1072-1079. doi: 10.1038/nm.4385. Epub 2017 Aug 21. Nat Med. 2017. PMID: 28825716 Free PMC article.
-
Cellular senescence in bone.Bone. 2019 Apr;121:121-133. doi: 10.1016/j.bone.2019.01.015. Epub 2019 Jan 16. Bone. 2019. PMID: 30659978 Free PMC article. Review.
-
The role of senolytics in osteoporosis and other skeletal pathologies.Mech Ageing Dev. 2021 Oct;199:111565. doi: 10.1016/j.mad.2021.111565. Epub 2021 Sep 6. Mech Ageing Dev. 2021. PMID: 34499959 Free PMC article. Review.
-
Independent Roles of Estrogen Deficiency and Cellular Senescence in the Pathogenesis of Osteoporosis: Evidence in Young Adult Mice and Older Humans.J Bone Miner Res. 2019 Aug;34(8):1407-1418. doi: 10.1002/jbmr.3729. Epub 2019 Jun 21. J Bone Miner Res. 2019. PMID: 30913313 Free PMC article.
-
The role of cellular senescence in ageing and endocrine disease.Nat Rev Endocrinol. 2020 May;16(5):263-275. doi: 10.1038/s41574-020-0335-y. Epub 2020 Mar 11. Nat Rev Endocrinol. 2020. PMID: 32161396 Free PMC article. Review.
Cited by
-
Identification and Analysis of Genes Underlying Bone Mineral Density by Integrating Microarray Data of Osteoporosis.Front Cell Dev Biol. 2020 Aug 27;8:798. doi: 10.3389/fcell.2020.00798. eCollection 2020. Front Cell Dev Biol. 2020. PMID: 32974344 Free PMC article.
-
BMP9 reduces age-related bone loss in mice by inhibiting osteoblast senescence through Smad1-Stat1-P21 axis.Cell Death Discov. 2022 May 6;8(1):254. doi: 10.1038/s41420-022-01048-8. Cell Death Discov. 2022. PMID: 35523787 Free PMC article.
-
The Spectrum of Fundamental Basic Science Discoveries Contributing to Organismal Aging.J Bone Miner Res. 2018 Sep;33(9):1568-1584. doi: 10.1002/jbmr.3564. Epub 2018 Aug 13. J Bone Miner Res. 2018. PMID: 30075061 Free PMC article. Review.
-
Osteoporosis and Sarcopenia Increase Frailty Syndrome in the Elderly.Front Endocrinol (Lausanne). 2019 Apr 24;10:255. doi: 10.3389/fendo.2019.00255. eCollection 2019. Front Endocrinol (Lausanne). 2019. PMID: 31068903 Free PMC article. Review.
-
Towards Healthy Longevity: Comprehensive Insights from Molecular Targets and Biomarkers to Biological Clocks.Int J Mol Sci. 2024 Jun 20;25(12):6793. doi: 10.3390/ijms25126793. Int J Mol Sci. 2024. PMID: 38928497 Free PMC article. Review.
References
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–1733. - PubMed
-
- Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int. 1997;7(5):407–413. - PubMed
-
- Cauley JA, Wampler NS, Barnhart JM, Wu L, Allison M, Chen Z, Hendrix S, Robbins J, Jackson RD; Women’s Health Initiative Observational Study . Incidence of fractures compared to cardiovascular disease and breast cancer: the Women’s Health Initiative Observational Study. Osteoporos Int. 2008;19(12):1717–1723. - PMC - PubMed
-
- Rossouw JE, Prentice RL, Manson JE, Wu L, Barad D, Barnabei VM, Ko M, LaCroix AZ, Margolis KL, Stefanick ML. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA. 2007;297(13):1465–1477. - PubMed
-
- Riggs BL, Hartmann LC. Selective estrogen-receptor modulators: mechanisms of action and application to clinical practice. N Engl J Med. 2003;348(7):618–629. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
