

Placental Morphology Is Associated with Maternal Depressive Symptoms during Pregnancy and Toddler Psychiatric Problems
- PMID: 29335435
- PMCID: PMC5768752
- DOI: 10.1038/s41598-017-19133-9
Placental Morphology Is Associated with Maternal Depressive Symptoms during Pregnancy and Toddler Psychiatric Problems
Abstract
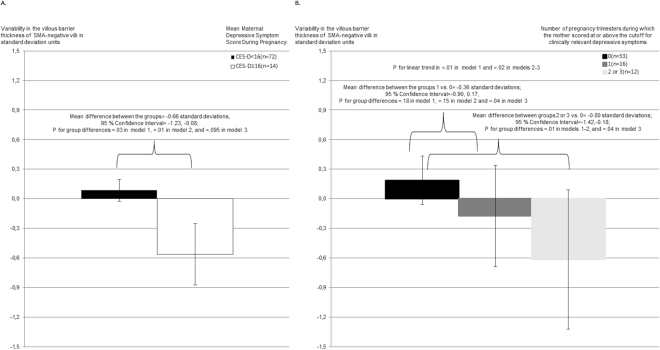
Maternal depressive symptoms during pregnancy predict increased psychiatric problems in children. The underlying biological mechanisms remain unclear. Hence, we examined whether alterations in the morphology of 88 term placentas were associated with maternal depressive symptoms during pregnancy and psychiatric problems in 1.9-3.1-years old (Mean = 2.1 years) toddlers. Maternal depressive symptoms were rated biweekly during pregnancy with the Center of Epidemiological Studies Depression Scale (n = 86). Toddler psychiatric problems were mother-rated with the Child Behavior Checklist (n = 60). We found that higher maternal depressive symptoms throughout pregnancy [B = -0.24 Standard Deviation (SD) units: 95% Confidence Interval (CI) = -0.46; -0.03: P = 0.03; Mean difference = -0.66 SDs; 95% CI = -0.08; -1.23: P = 0.03; between those with and without clinically relevant depressive symptoms] were associated with lower variability in the placental villous barrier thickness of γ-smooth muscle actin-negative villi. This placental morphological change predicted higher total (B = -0.34 SDs: 95% CI = -0.60; -0.07: P = 0.01) and internalizing (B = -0.32 SDs: 95% CI = -0.56; -0.08: P = 0.01) psychiatric problems in toddlers. To conclude, our findings suggest that both maternal depressive symptoms during pregnancy and toddler psychiatric problems may be associated with lower variability in the villous membrane thickness of peripheral villi in term placentas. This lower heterogeneity may compromise materno-fetal exchange, suggesting a possible role for altered placental morphology in the fetal programming of mental disorders.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Maternal Depressive Symptoms During and After Pregnancy and Psychiatric Problems in Children.J Am Acad Child Adolesc Psychiatry. 2017 Jan;56(1):30-39.e7. doi: 10.1016/j.jaac.2016.10.007. Epub 2016 Oct 24. J Am Acad Child Adolesc Psychiatry. 2017. PMID: 27993226
-
Infant regulatory behavior problems during first month of life and neurobehavioral outcomes in early childhood.Eur Child Adolesc Psychiatry. 2019 Jun;28(6):847-859. doi: 10.1007/s00787-018-1243-8. Epub 2018 Nov 3. Eur Child Adolesc Psychiatry. 2019. PMID: 30392118 Free PMC article.
-
Maternal depressive symptoms: associations with adolescents' internalizing and externalizing problems and social competence.Nord J Psychiatry. 2014 Jul;68(5):323-32. doi: 10.3109/08039488.2013.838804. Epub 2013 Sep 27. Nord J Psychiatry. 2014. PMID: 24070429
-
Maternal prenatal stress and postnatal depressive symptoms: discrepancy between mother and teacher reports of toddler psychological problems.Soc Psychiatry Psychiatr Epidemiol. 2021 Apr;56(4):559-570. doi: 10.1007/s00127-020-01964-z. Epub 2020 Sep 29. Soc Psychiatry Psychiatr Epidemiol. 2021. PMID: 32995941 Free PMC article.
-
Pathophysiology of placental-derived fetal growth restriction.Am J Obstet Gynecol. 2018 Feb;218(2S):S745-S761. doi: 10.1016/j.ajog.2017.11.577. Am J Obstet Gynecol. 2018. PMID: 29422210 Review.
Cited by
-
The Placentas of Women Who Suffer an Episode of Psychosis during Pregnancy Have Increased Lipid Peroxidation with Evidence of Ferroptosis.Biomolecules. 2023 Jan 6;13(1):120. doi: 10.3390/biom13010120. Biomolecules. 2023. PMID: 36671505 Free PMC article.
-
Women with psychotic episodes during pregnancy show increased markers of placental damage with Tenney-Parker changes.Histol Histopathol. 2023 Oct;38(10):1109-1118. doi: 10.14670/HH-18-605. Epub 2023 Mar 7. Histol Histopathol. 2023. PMID: 36916695
-
The Density of Cell Nuclei at the Materno-Fetal Exchange Barrier is Sexually Dimorphic in Normal Placentas, but not in IUGR.Sci Rep. 2019 Feb 20;9(1):2359. doi: 10.1038/s41598-019-38739-9. Sci Rep. 2019. PMID: 30787322 Free PMC article.
-
A polyepigenetic glucocorticoid exposure score at birth and childhood mental and behavioral disorders.Neurobiol Stress. 2020 Nov 21;13:100275. doi: 10.1016/j.ynstr.2020.100275. eCollection 2020 Nov. Neurobiol Stress. 2020. PMID: 33344728 Free PMC article.
-
The Consequences of Assisted Reproduction Technologies on the Offspring Health Throughout Life: A Placental Contribution.Front Cell Dev Biol. 2022 May 20;10:906240. doi: 10.3389/fcell.2022.906240. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 35747691 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
