

1.5 Tesla Magnetic Resonance Imaging to Investigate Potential Etiologies of Brain Swelling in Pediatric Cerebral Malaria
- PMID: 29313473
- PMCID: PMC5929182
- DOI: 10.4269/ajtmh.17-0309
1.5 Tesla Magnetic Resonance Imaging to Investigate Potential Etiologies of Brain Swelling in Pediatric Cerebral Malaria
Abstract
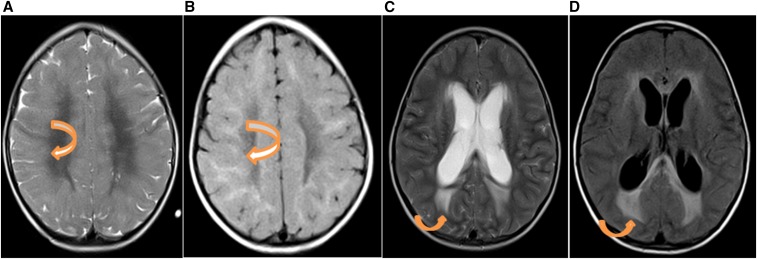
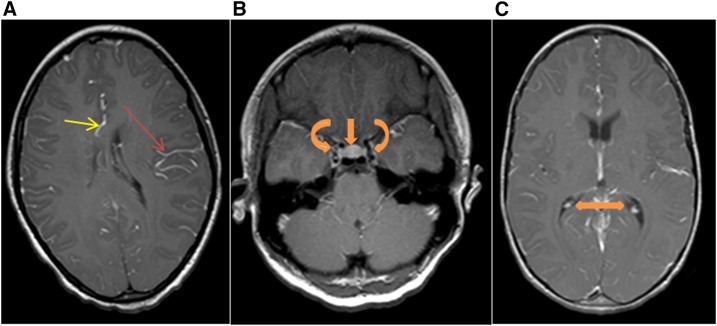
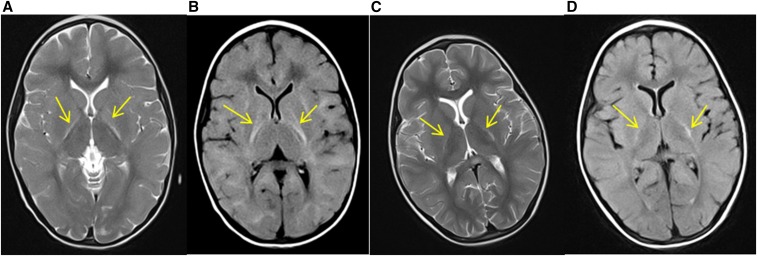
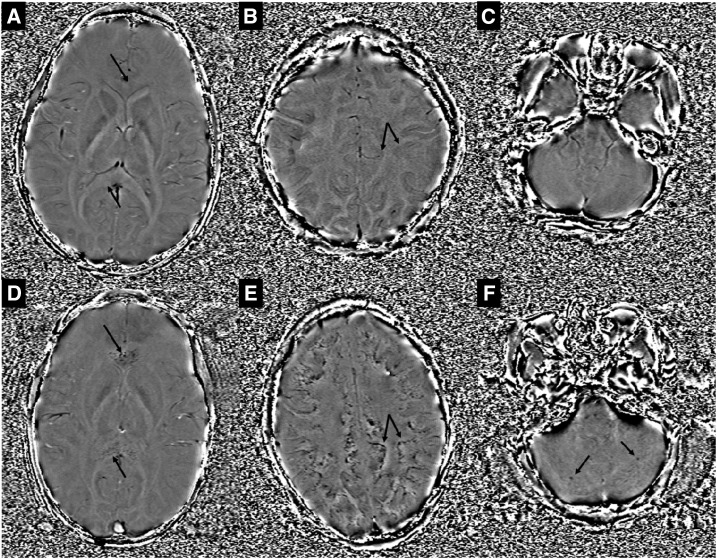
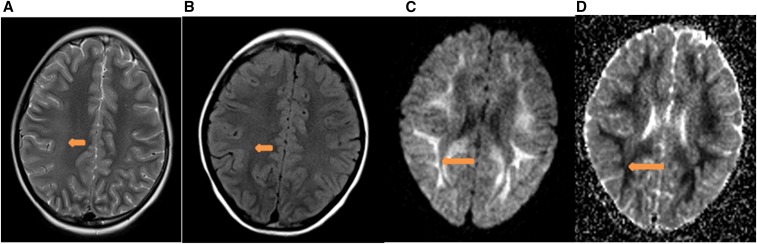
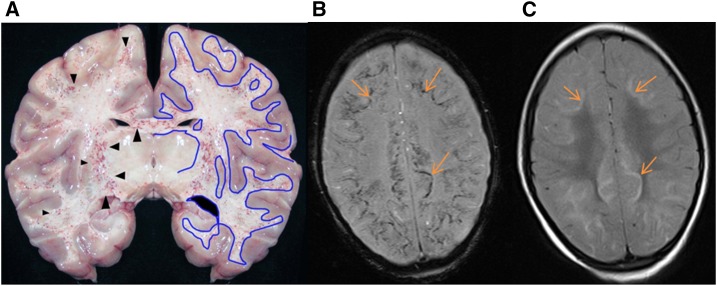
The hallmark of pediatric cerebral malaria (CM) is sequestration of parasitized red blood cells in the cerebral microvasculature. Malawi-based research using 0.35 Tesla (T) magnetic resonance imaging (MRI) established that severe brain swelling is associated with fatal CM, but swelling etiology remains unclear. Autopsy and clinical studies suggest several potential etiologies, but limitations of 0.35 T MRI precluded optimal investigations into swelling pathophysiology. A 1.5 T MRI in Zambia allowed for further investigations including susceptibility-weighted imaging (SWI). SWI is an ideal sequence for identifying regions of sequestration and microhemorrhages given the ferromagnetic properties of hemozoin and blood. Using 1.5 T MRI, Zambian children with retinopathy-confirmed CM underwent imaging with SWI, T2, T1 pre- and post-gadolinium, diffusion-weighted imaging (DWI) with apparent diffusion coefficients and T2/fluid attenuated inversion recovery sequences. Sixteen children including two with moderate/severe edema were imaged; all survived. Gadolinium extravasation was not seen. DWI abnormalities spared the gray matter suggesting vasogenic edema with viable tissue rather than cytotoxic edema. SWI findings consistent with microhemorrhages and parasite sequestration co-occurred in white matter regions where DWI changes consistent with vascular congestion were seen. Imaging findings consistent with posterior reversible encephalopathy syndrome were seen in children who subsequently had a rapid clinical recovery. High field MRI indicates that vascular congestion associated with parasite sequestration, local inflammation from microhemorrhages and autoregulatory dysfunction likely contribute to brain swelling in CM. No gross radiological blood brain barrier breakdown or focal cortical DWI abnormalities were evident in these children with nonfatal CM.
Figures
Similar articles
-
Magnetic Resonance Imaging of Cerebral Malaria Patients Reveals Distinct Pathogenetic Processes in Different Parts of the Brain.mSphere. 2017 Jun 7;2(3):e00193-17. doi: 10.1128/mSphere.00193-17. eCollection 2017 May-Jun. mSphere. 2017. PMID: 28596990 Free PMC article.
-
Severity of retinopathy parallels the degree of parasite sequestration in the eyes and brains of malawian children with fatal cerebral malaria.J Infect Dis. 2015 Jun 15;211(12):1977-86. doi: 10.1093/infdis/jiu592. Epub 2014 Oct 28. J Infect Dis. 2015. PMID: 25351204 Free PMC article.
-
Brain MRI of children with retinopathy-negative cerebral malaria.Am J Trop Med Hyg. 2014 Nov;91(5):943-9. doi: 10.4269/ajtmh.14-0216. Epub 2014 Sep 8. Am J Trop Med Hyg. 2014. PMID: 25200262 Free PMC article.
-
Magnetic resonance susceptibility weighted imaging in neurosurgery: current applications and future perspectives.J Neurosurg. 2015 Dec;123(6):1463-75. doi: 10.3171/2015.1.JNS142349. Epub 2015 Jul 24. J Neurosurg. 2015. PMID: 26207600 Review.
-
Brain magnetic resonance in status epilepticus: A focused review.Seizure. 2016 May;38:63-7. doi: 10.1016/j.seizure.2016.04.007. Epub 2016 Apr 23. Seizure. 2016. PMID: 27156207 Review.
Cited by
-
The Ins and Outs of Cerebral Malaria Pathogenesis: Immunopathology, Extracellular Vesicles, Immunometabolism, and Trained Immunity.Front Immunol. 2019 Apr 17;10:830. doi: 10.3389/fimmu.2019.00830. eCollection 2019. Front Immunol. 2019. PMID: 31057552 Free PMC article. Review.
-
Brain magnetic resonance imaging in imported malaria.Malar J. 2019 Mar 12;18(1):74. doi: 10.1186/s12936-019-2713-2. Malar J. 2019. PMID: 30871543 Free PMC article.
-
Mechanisms of Transcranial Doppler Ultrasound phenotypes in paediatric cerebral malaria remain elusive.Malar J. 2022 Jun 21;21(1):196. doi: 10.1186/s12936-022-04163-0. Malar J. 2022. PMID: 35729574 Free PMC article.
-
Cerebral Malaria and Neuronal Implications of Plasmodium Falciparum Infection: From Mechanisms to Advanced Models.Adv Sci (Weinh). 2022 Dec;9(36):e2202944. doi: 10.1002/advs.202202944. Epub 2022 Oct 27. Adv Sci (Weinh). 2022. PMID: 36300890 Free PMC article. Review.
-
Pediatric Cerebral Malaria.Curr Trop Med Rep. 2021 Jun;8(2):69-80. doi: 10.1007/s40475-021-00227-4. Epub 2021 Jan 25. Curr Trop Med Rep. 2021. PMID: 34150445 Free PMC article. No abstract available.
References
-
- WHO , 2011. World Malaria Report. Geneva, Switzerland: World Health Organization.
-
- Molyneux ME, Taylor TE, Wirima JJ, Borgstein A, 1989. Clinical features and prognostic indicators in paediatric cerebral malaria: a study of 131 comatose Malawian children. Q J Med 71: 441–459. - PubMed
-
- Paul F, Roath S, Melville D, Warhurst DC, Osisanya JO, 1981. Separation of malaria-infected erythrocytes from whole blood: use of a selective high-gradient magnetic separation technique. Lancet 2: 70–71. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
