

Inhibition of Tissue Matrix Metalloproteinases Interferes with Mycobacterium tuberculosis-Induced Granuloma Formation and Reduces Bacterial Load in a Human Lung Tissue Model
- PMID: 29259583
- PMCID: PMC5723394
- DOI: 10.3389/fmicb.2017.02370
Inhibition of Tissue Matrix Metalloproteinases Interferes with Mycobacterium tuberculosis-Induced Granuloma Formation and Reduces Bacterial Load in a Human Lung Tissue Model
Abstract
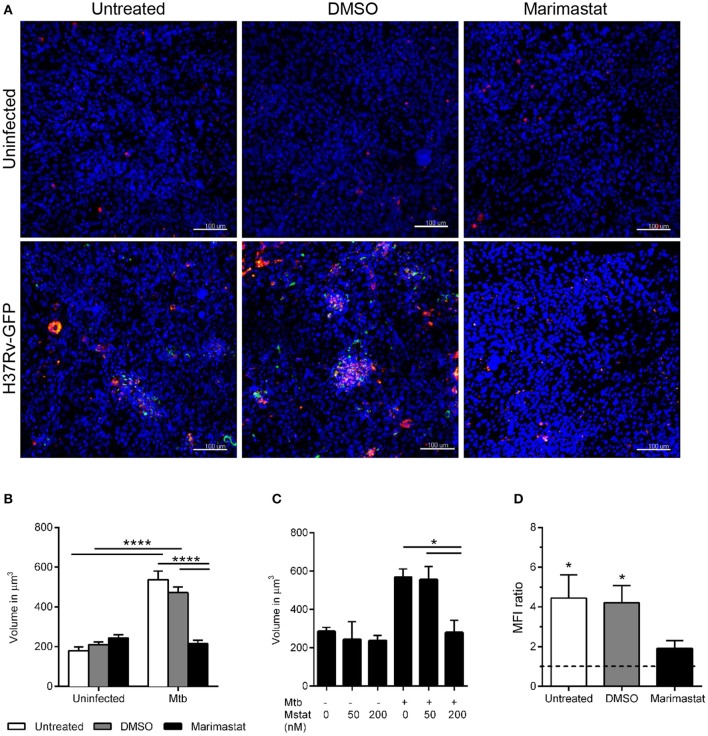
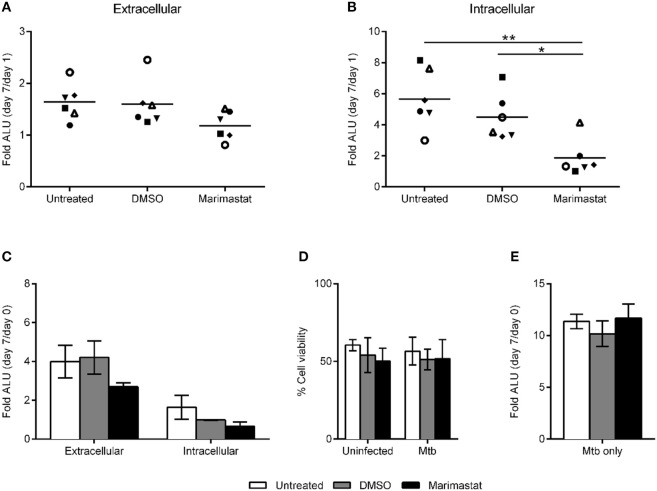
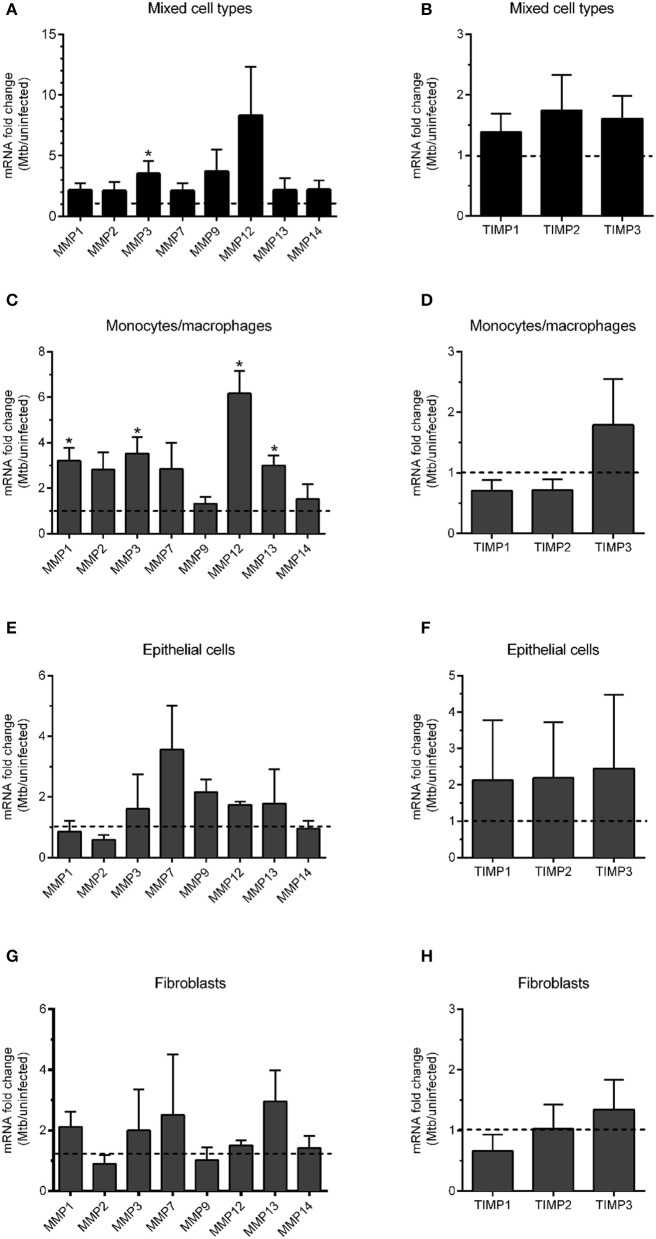
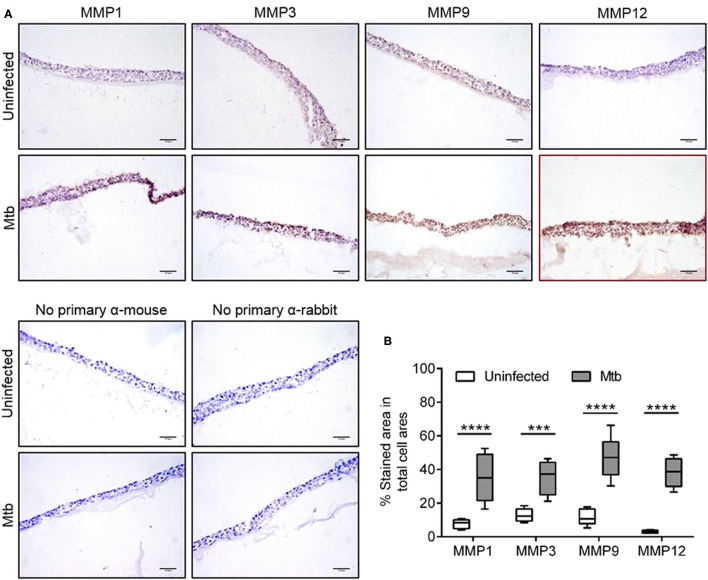
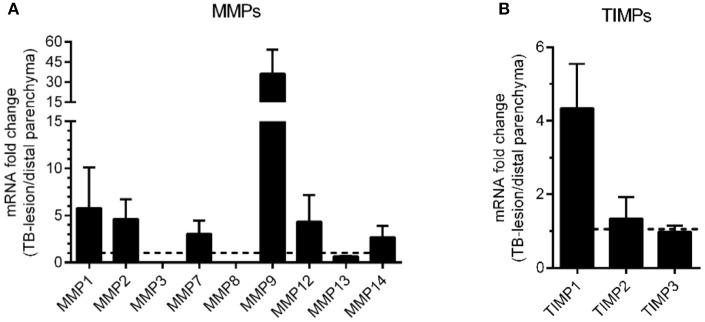
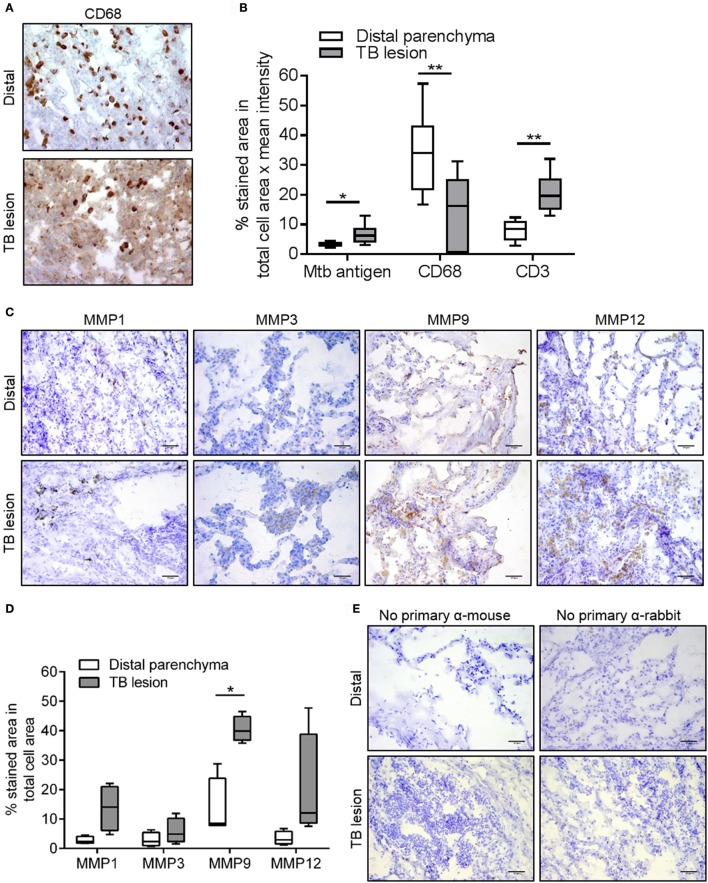
Granulomas are hallmarks of pulmonary tuberculosis (TB) and traditionally viewed as host-protective structures. However, recent evidence suggest that Mycobacterium tuberculosis (Mtb) uses its virulence factors to stimulate the formation of granuloma. In the present study, we investigated the contribution of matrix metalloproteinases (MMPs), host enzymes that cause degradation of the extracellular matrix, to granuloma formation and bacterial load in Mtb-infected tissue. To this end, we used our lung tissue model for TB, which is based on human lung-derived cells and primary human monocyte-derived macrophages. Global inhibition of MMPs in the Mtb-infected tissue model reduced both granuloma formation and bacterial load. The infection caused upregulation of a set of MMPs (MMP1, 3, 9, and 12), and this finding could be validated in lung biopsies from patients with non-cavitary TB. Data from this study indicate that MMP activation contributes to early TB granuloma formation, suggesting that host-directed, MMP-targeted intervention could be considered as adjunct therapy to TB treatment.
Keywords: granuloma; matrix metalloproteinases; tissue inhibitor of matrix metalloproteinases; tissue models; tuberculosis.
Figures
Similar articles
-
Breaking the Cycle: Matrix Metalloproteinase Inhibitors as an Alternative Approach in Managing Tuberculosis Pathogenesis and Progression.ACS Infect Dis. 2024 Aug 9;10(8):2567-2583. doi: 10.1021/acsinfecdis.4c00385. Epub 2024 Jul 22. ACS Infect Dis. 2024. PMID: 39038212 Review.
-
Matrix metalloproteinases: Expression, regulation and role in the immunopathology of tuberculosis.Cell Prolif. 2019 Jul;52(4):e12649. doi: 10.1111/cpr.12649. Epub 2019 Jun 14. Cell Prolif. 2019. PMID: 31199047 Free PMC article. Review.
-
Modeling Mycobacterium tuberculosis early granuloma formation in experimental human lung tissue.Dis Model Mech. 2014 Feb;7(2):281-8. doi: 10.1242/dmm.013854. Epub 2013 Nov 7. Dis Model Mech. 2014. PMID: 24203885 Free PMC article.
-
A matrix metalloproteinase inhibitor promotes granuloma formation during the early phase of Mycobacterium tuberculosis pulmonary infection.Tuberculosis (Edinb). 2004;84(6):387-96. doi: 10.1016/j.tube.2004.07.001. Tuberculosis (Edinb). 2004. PMID: 15525562
-
Identifying mechanisms driving formation of granuloma-associated fibrosis during Mycobacterium tuberculosis infection.J Theor Biol. 2017 Sep 21;429:1-17. doi: 10.1016/j.jtbi.2017.06.017. Epub 2017 Jun 20. J Theor Biol. 2017. PMID: 28642013 Free PMC article.
Cited by
-
A Modular Microscale Granuloma Model for Immune-Microenvironment Signaling Studies in vitro.Front Bioeng Biotechnol. 2020 Aug 18;8:931. doi: 10.3389/fbioe.2020.00931. eCollection 2020. Front Bioeng Biotechnol. 2020. PMID: 32974300 Free PMC article.
-
Host and Pathogen Communication in the Respiratory Tract: Mechanisms and Models of a Complex Signaling Microenvironment.Front Med (Lausanne). 2020 Sep 10;7:537. doi: 10.3389/fmed.2020.00537. eCollection 2020. Front Med (Lausanne). 2020. PMID: 33015094 Free PMC article. Review.
-
Doxycycline host-directed therapy in human pulmonary tuberculosis.J Clin Invest. 2021 Aug 2;131(15):e141895. doi: 10.1172/JCI141895. J Clin Invest. 2021. PMID: 34128838 Free PMC article. Clinical Trial.
-
Matrix Metalloproteinases and Tissue Inhibitors of Metalloproteinases Are Potential Biomarkers of Pulmonary and Extra-Pulmonary Tuberculosis.Front Immunol. 2020 Mar 11;11:419. doi: 10.3389/fimmu.2020.00419. eCollection 2020. Front Immunol. 2020. PMID: 32218787 Free PMC article.
-
Host-Directed Therapies: Modulating Inflammation to Treat Tuberculosis.Front Immunol. 2021 Apr 19;12:660916. doi: 10.3389/fimmu.2021.660916. eCollection 2021. Front Immunol. 2021. PMID: 33953722 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources