

S100A8/A9 and sRAGE kinetic after polytrauma; an explorative observational study
- PMID: 29178941
- PMCID: PMC5702249
- DOI: 10.1186/s13049-017-0455-0
S100A8/A9 and sRAGE kinetic after polytrauma; an explorative observational study
Abstract
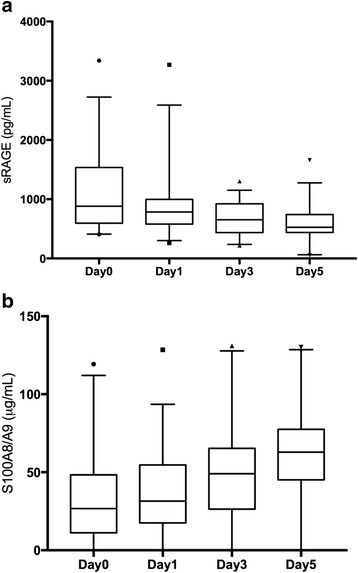
Background: Following tissue injury after trauma, the activation of innate immune pathways results in systemic inflammation, organ failure and an increased risk of infections. The objective of this study was to characterize the kinetics of the S100A8/S100A9 complex, a new-recognized alarmin, as well as its soluble receptor sRAGE, over time after trauma as potential early biomarkers of the risk of organ damage.
Methods: We collected comprehensive data from consenting patients admitted to an ICU following severe trauma. The blood samples were taken at Day 0 (admission), Day1, 3 and 5 S100A8/A9 and sRAGE were measured by ELISA. Biomarkers levels were reported as median (IQR).
Results: Thirty-eight patients sustaining in majority a blunt trauma (89%) with a median ISS of 39 were included. In this cohort, the S100A8/A9 complex increased significantly over time (p = 0.001), but its levels increment over time (D0 to D5) was significantly smaller in patients developing infection (7.6 vs 40.1 mcg/mL, p = 0.011). The circulating level of sRAGE circulating levels decreased over time (p < 0.0001) and was higher in patients who remained in shock on day 3 (550 vs 918 pg/mL; p = 0.02) or 5 (498 vs 644 pg/mL; p = 0.045). Admission sRAGE levels were significantly higher in non-survivors (1694 vs 745 pg/mL; p = 0.015) and was higher in patients developing renal failure (1143 vs 696 pg/mL, p = 0.011).
Discussion: Our findings reveal an interesting association between the biomarker S100A8/9 least increase over time and the presence of infectious complication after trauma. We describe that the sRAGE decline over time is in relation with shock and markers of ischemic injury. We also confirm the association of sRAGE levels measured at admission with mortality and the development of renal failure.
Conclusions: This work illustrates the importance of following the circulating level of biomarker overtime. The utilization of S1008/9 as a tool to stratify infection risk and trigger early interventions need to be validated prospectively.
Keywords: Calgranulines; Infection; Inflammation; Organ failure; S100; Trauma; sRAGE.
Conflict of interest statement
Ethics approval and consent to participate
The local Institutional Research Ethics Board approved the study (REB#09–183), and approved a delayed consent model. Written informed consent was obtained from the legally authorized representative within 72 h or the trauma and from the patient him/herself when capacity had recovered.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Serum levels of soluble receptor for advanced glycation end products and of S100 proteins are associated with inflammatory, autoantibody, and classical risk markers of joint and vascular damage in rheumatoid arthritis.Arthritis Res Ther. 2009;11(2):R39. doi: 10.1186/ar2645. Epub 2009 Mar 11. Arthritis Res Ther. 2009. PMID: 19284577 Free PMC article.
-
Differential Regulation of Circulating Soluble Receptor for Advanced Glycation End Products (sRAGEs) and Its Ligands S100A8/A9 Four Weeks Post an Exercise Intervention in a Cohort of Young Army Recruits.Biomolecules. 2021 Sep 13;11(9):1354. doi: 10.3390/biom11091354. Biomolecules. 2021. PMID: 34572568 Free PMC article. Clinical Trial.
-
Circulating S100A8/A9 Levels Reflect Intraocular Inflammation in Uveitis Patients.Ocul Immunol Inflamm. 2020;28(1):133-141. doi: 10.1080/09273948.2018.1538461. Epub 2018 Nov 5. Ocul Immunol Inflamm. 2020. PMID: 30395736
-
S100A8 and S100A9: DAMPs at the crossroads between innate immunity, traditional risk factors, and cardiovascular disease.Mediators Inflamm. 2013;2013:828354. doi: 10.1155/2013/828354. Epub 2013 Dec 22. Mediators Inflamm. 2013. PMID: 24453429 Free PMC article. Review.
-
S100A8/A9 as a biomarker for synovial inflammation and joint damage in patients with rheumatoid arthritis.Korean J Intern Med. 2014 Jan;29(1):12-9. doi: 10.3904/kjim.2014.29.1.12. Epub 2014 Jan 2. Korean J Intern Med. 2014. PMID: 24574827 Free PMC article. Review.
Cited by
-
Therapeutic Potential of Mesenchymal Stromal Cell-Derived Extracellular Vesicles in the Prevention of Organ Injuries Induced by Traumatic Hemorrhagic Shock.Front Immunol. 2021 Sep 29;12:749659. doi: 10.3389/fimmu.2021.749659. eCollection 2021. Front Immunol. 2021. PMID: 34659252 Free PMC article. Review.
-
Calprotectin and Calgranulin C as Biomarkers of Pancreatic Tumors: Baseline Levels and Level Changes after Surgery.Mediators Inflamm. 2019 Sep 9;2019:6985703. doi: 10.1155/2019/6985703. eCollection 2019. Mediators Inflamm. 2019. PMID: 31582902 Free PMC article.
-
Platelet dysfunction after trauma: From mechanisms to targeted treatment.Transfusion. 2022 Aug;62 Suppl 1(Suppl 1):S281-S300. doi: 10.1111/trf.16971. Epub 2022 Jun 24. Transfusion. 2022. PMID: 35748694 Free PMC article. Review. No abstract available.
-
The immune suppressive properties of damage associated molecular patterns in the setting of sterile traumatic injury.Front Immunol. 2023 Aug 15;14:1239683. doi: 10.3389/fimmu.2023.1239683. eCollection 2023. Front Immunol. 2023. PMID: 37662933 Free PMC article. Review.
-
Exploratory Investigation of the Plasma Proteome Associated with the Endotheliopathy of Trauma.Int J Mol Sci. 2022 Jun 1;23(11):6213. doi: 10.3390/ijms23116213. Int J Mol Sci. 2022. PMID: 35682894 Free PMC article.
References
-
- Frohlich M, Lefering R, Probst C, Paffrath T, Schneider MM, Maegele M, et al. Epidemiology and risk factors of multiple-organ failure after multiple trauma: an analysis of 31,154 patients from the TraumaRegister DGU. J Trauma Acute Care Surgery. 2014;76:921–7–discussion927–8. - PubMed
-
- Wafaisade A, Lefering R, Bouillon B, Sakka SG, Thamm OC, Paffrath T, et al. Epidemiology and risk factors of sepsis after multiple trauma: an analysis of 29,829 patients from the trauma registry of the German Society for Trauma Surgery. Crit Care Med. 2011;39:621–628. doi: 10.1097/CCM.0b013e318206d3df. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
