

Diabetes and Sepsis: Risk, Recurrence, and Ruination
- PMID: 29163354
- PMCID: PMC5670360
- DOI: 10.3389/fendo.2017.00271
Diabetes and Sepsis: Risk, Recurrence, and Ruination
Abstract
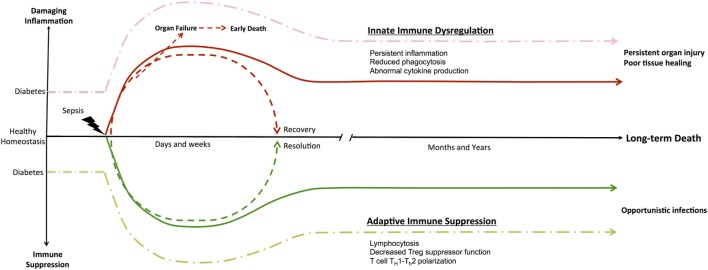
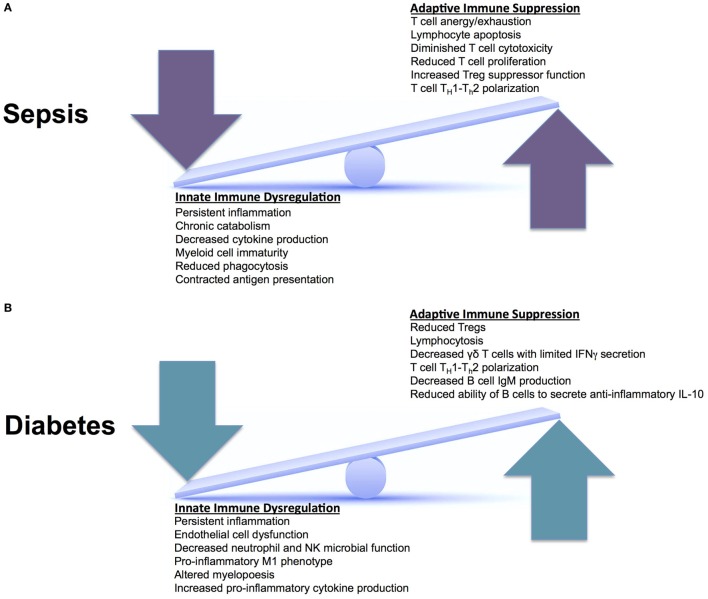
Sepsis develops when an infection surpasses local tissue containment. A series of dysregulated physiological responses are generated, leading to organ dysfunction and a 10% mortality risk. When patients with sepsis demonstrate elevated serum lactates and require vasopressor therapy to maintain adequate blood pressure in the absence of hypovolemia, they are in septic shock with an in-hospital mortality rate >40%. With improvements in intensive care treatment strategies, overall sepsis mortality has diminished to ~20% at 30 days; however, mortality continues to steadily climb after recovery from the acute event. Traditionally, it was thought that the complex interplay between inflammatory and anti-inflammatory responses led to sepsis-induced organ dysfunction and mortality. However, a closer examination of those who die long after sepsis subsides reveals that many initial survivors succumb to recurrent, nosocomial, and secondary infections. The comorbidly challenged, physiologically frail diabetic individuals suffer the highest infection rates. Recent reports suggest that even after clinical "recovery" from sepsis, persistent alterations in innate and adaptive immune responses exists resulting in chronic inflammation, immune suppression, and bacterial persistence. As sepsis-associated immune defects are associated with increased mortality long-term, a potential exists for immune modulatory therapy to improve patient outcomes. We propose that diabetes causes a functional immune deficiency that directly reduces immune cell function. As a result, patients display diminished bactericidal clearance, increased infectious complications, and protracted sepsis mortality. Considering the substantial expansion of the elderly and obese population, global adoption of a Western diet and lifestyle, and multidrug resistant bacterial emergence and persistence, diabetic mortality from sepsis is predicted to rise dramatically over the next two decades. A better understanding of the underlying diabetic-induced immune cell defects that persist following sepsis are crucial to identify potential therapeutic targets to bolster innate and adaptive immune function, prevent infectious complications, and provide more durable diabetic survival.
Keywords: complications; diabetes; infections; resource utilization; sepsis; septic shock.
Figures
Similar articles
-
The immune system's role in sepsis progression, resolution, and long-term outcome.Immunol Rev. 2016 Nov;274(1):330-353. doi: 10.1111/imr.12499. Immunol Rev. 2016. PMID: 27782333 Free PMC article. Review.
-
Sepsis Care Pathway 2019.Qatar Med J. 2019 Nov 7;2019(2):4. doi: 10.5339/qmj.2019.qccc.4. eCollection 2019. Qatar Med J. 2019. PMID: 31763206 Free PMC article.
-
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012.Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af. Crit Care Med. 2013. PMID: 23353941
-
Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012.Intensive Care Med. 2013 Feb;39(2):165-228. doi: 10.1007/s00134-012-2769-8. Epub 2013 Jan 30. Intensive Care Med. 2013. PMID: 23361625 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Care pathways of sepsis survivors: sequelae, mortality and use of healthcare services in France, 2015-2018.Crit Care. 2023 Nov 10;27(1):438. doi: 10.1186/s13054-023-04726-w. Crit Care. 2023. PMID: 37950254 Free PMC article.
-
Cost-Effectiveness of Insulin Glargine and Insulin Detemir in the Basal Regimen for Naïve Insulin Patients with Type 2 Diabetes Mellitus (T2DM) in Malaysia.Clinicoecon Outcomes Res. 2020 Jun 22;12:333-343. doi: 10.2147/CEOR.S244884. eCollection 2020. Clinicoecon Outcomes Res. 2020. PMID: 32606850 Free PMC article.
-
Predictive nomogram model for major adverse kidney events within 30 days in sepsis patients with type 2 diabetes mellitus.Front Endocrinol (Lausanne). 2022 Dec 16;13:1024500. doi: 10.3389/fendo.2022.1024500. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36589822 Free PMC article.
-
The diabetes pandemic and associated infections: suggestions for clinical microbiology.Rev Med Microbiol. 2019 Jan;30(1):1-17. doi: 10.1097/MRM.0000000000000155. Epub 2018 Nov 1. Rev Med Microbiol. 2019. PMID: 30662163 Free PMC article.
-
Monocyte subtype expression patterns in septic patients with diabetes are distinct from patterns observed in obese patients.Front Med (Lausanne). 2023 Jan 5;9:1026298. doi: 10.3389/fmed.2022.1026298. eCollection 2022. Front Med (Lausanne). 2023. PMID: 36687421 Free PMC article.
References
-
- Martin GS, Mannino DM, Moss M. The effect of age on the development and outcome of adult sepsis. Crit Care Med (2006) 34:15–21.10.1097/01.CCM.0000194535.82812.BA - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials