

Evaluation of Different Parameters of Humoral and Cellular Immune Responses in HIV Serodiscordant Heterosexual Couples: Humoral Response Potentially Implicated in Modulating Transmission Rates
- PMID: 29129698
- PMCID: PMC5832641
- DOI: 10.1016/j.ebiom.2017.11.001
Evaluation of Different Parameters of Humoral and Cellular Immune Responses in HIV Serodiscordant Heterosexual Couples: Humoral Response Potentially Implicated in Modulating Transmission Rates
Abstract
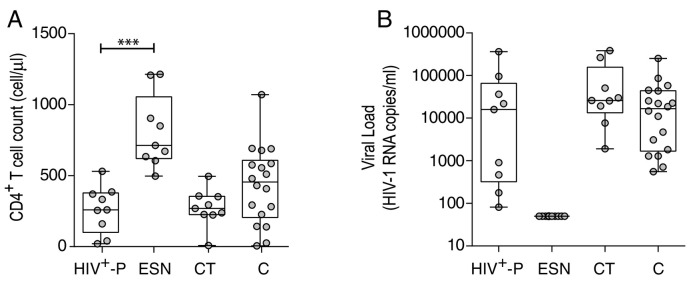
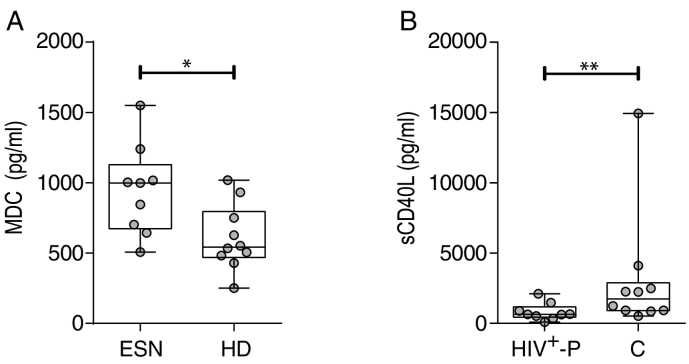
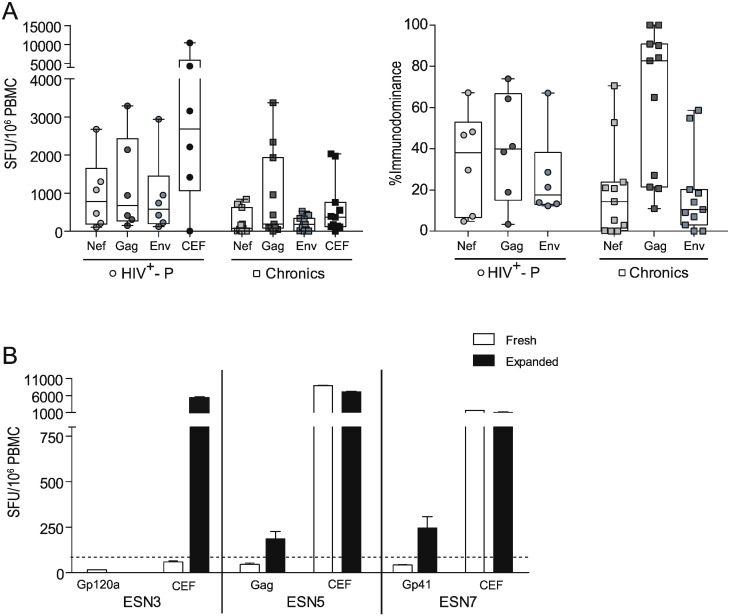
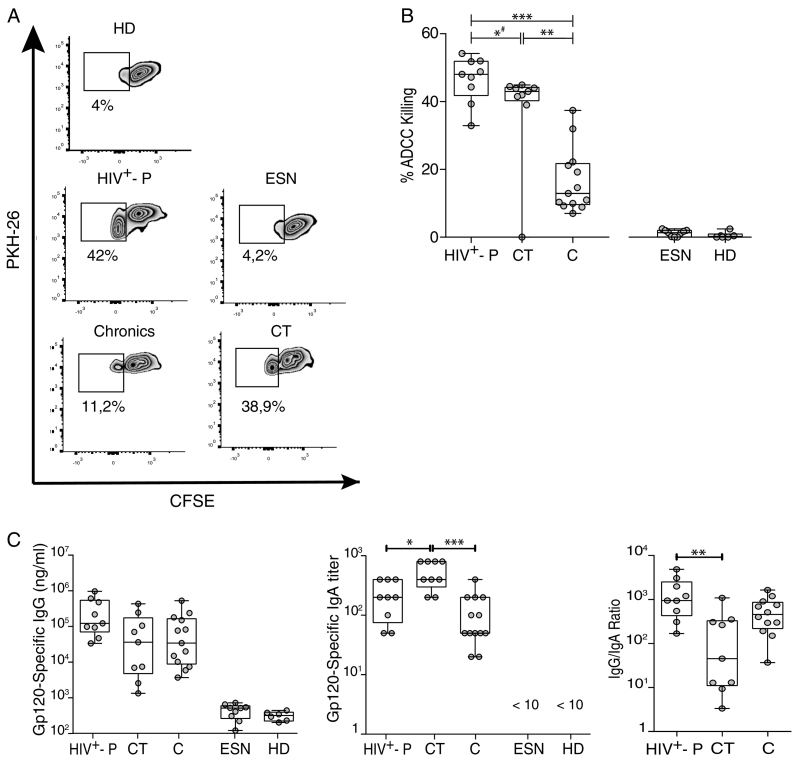
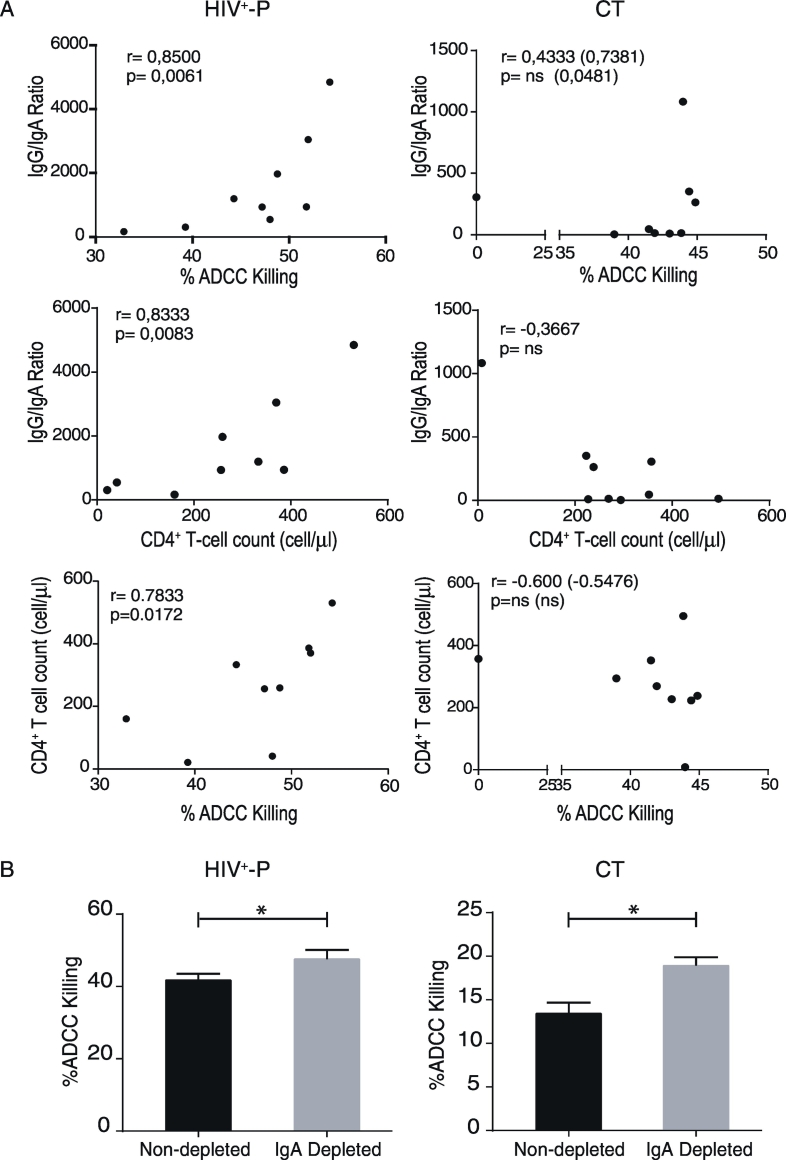
As the HIV/AIDS pandemic still progresses, understanding the mechanisms governing viral transmission as well as protection from HIV acquisition is fundamental. In this context, cohorts of HIV serodiscordant heterosexual couples (SDC) represent a unique tool. The present study was aimed to evaluate specific parameters of innate, cellular and humoral immune responses in SDC. Specifically, plasma levels of cytokines and chemokines, HIV-specific T-cell responses, gp120-specific IgG and IgA antibodies, and HIV-specific antibody-dependent cellular cytotoxicity (ADCC) activity were assessed in nine HIV-exposed seronegative individuals (ESN) and their corresponding HIV seropositive partners (HIV+-P), in eighteen chronically infected HIV subjects (C), nine chronically infected subjects known to be HIV transmitters (CT) and ten healthy HIV- donors (HD). Very low magnitude HIV-specific cellular responses were found in two out of six ESN. Interestingly, HIV+-P had the highest ADCC magnitude, the lowest IgA levels and the highest IgG/IgA ratio, all compared to CT. Positive correlations between CD4+ T-cell counts and both IgG/IgA ratios and %ADCC killing uniquely distinguished HIV+-P. Additionally, evidence of IgA interference with ADCC responses from HIV+-P and CT is provided. These data suggest for the first time a potential role of ADCC and/or gp120-specific IgG/IgA balance in modulating heterosexual transmission. In sum, this study provides key information to understand the host factors that influence viral transmission, which should be considered in both the development of prophylactic vaccines and novel immunotherapies for HIV-1 infection.
Keywords: ADCC; HIV-1; HIV-1 transmission; Serodiscordant couples.
Copyright © 2017 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
A Role for Fc-Mediated Humoral Immunity in Reducing HIV Transmission Rates between HIV Serodiscordant Heterosexual Couples.EBioMedicine. 2017 Dec;26:2-3. doi: 10.1016/j.ebiom.2017.11.011. Epub 2017 Nov 16. EBioMedicine. 2017. PMID: 29174161 Free PMC article. No abstract available.
Similar articles
-
Env-Specific IgA from Viremic HIV-Infected Subjects Compromises Antibody-Dependent Cellular Cytotoxicity.J Virol. 2016 Jan 15;90(2):670-81. doi: 10.1128/JVI.02363-15. Print 2016 Jan 15. J Virol. 2016. PMID: 26491172 Free PMC article.
-
HIV exposed seronegative individuals show antibodies specifically recognizing native HIV envelope glycoprotein.AIDS. 2013 Jun 1;27(9):1375-85. doi: 10.1097/QAD.0b013e32835fac08. AIDS. 2013. PMID: 23945502
-
Immune Correlates of Disease Progression in Linked HIV-1 Infection.Front Immunol. 2019 May 14;10:1062. doi: 10.3389/fimmu.2019.01062. eCollection 2019. Front Immunol. 2019. PMID: 31139189 Free PMC article.
-
Natural Immunity to HIV: A Template for Vaccine Strategies.Viruses. 2018 Apr 23;10(4):215. doi: 10.3390/v10040215. Viruses. 2018. PMID: 29690575 Free PMC article. Review.
-
Prospects for a globally effective HIV-1 vaccine.Vaccine. 2015 Nov 27;33 Suppl 4:D4-12. doi: 10.1016/j.vaccine.2015.03.059. Epub 2015 Jun 20. Vaccine. 2015. PMID: 26100921 Review.
Cited by
-
Recent insights into Fc-mediated effector responses to HIV-1.Curr Opin HIV AIDS. 2020 Sep;15(5):282-289. doi: 10.1097/COH.0000000000000638. Curr Opin HIV AIDS. 2020. PMID: 32675573 Free PMC article. Review.
-
Innate and Adaptive Anti-SIV Responses in Macaque Semen: Implications for Infectivity and Risk of Transmission.Front Immunol. 2020 May 12;11:850. doi: 10.3389/fimmu.2020.00850. eCollection 2020. Front Immunol. 2020. PMID: 32528466 Free PMC article.
-
Antibody-dependent cellular cytotoxicity targeting CD4-inducible epitopes predicts mortality in HIV-infected infants.EBioMedicine. 2019 Sep;47:257-268. doi: 10.1016/j.ebiom.2019.08.072. EBioMedicine. 2019. PMID: 31501077 Free PMC article.
-
Phenotype, Polyfunctionality, and Antiviral Activity of in vitro Stimulated CD8+ T-Cells From HIV+ Subjects Who Initiated cART at Different Time-Points After Acute Infection.Front Immunol. 2018 Oct 23;9:2443. doi: 10.3389/fimmu.2018.02443. eCollection 2018. Front Immunol. 2018. PMID: 30405632 Free PMC article.
-
Improved HIV-positive infant survival is correlated with high levels of HIV-specific ADCC activity in multiple cohorts.Cell Rep Med. 2021 Apr 20;2(4):100254. doi: 10.1016/j.xcrm.2021.100254. eCollection 2021 Apr 20. Cell Rep Med. 2021. PMID: 33948582 Free PMC article.
References
-
- Addo M.M., Altfeld M., Brainard D.M., Rathod A., Piechocka-Trocha A., Fideli U., Mulenga J., Shutes E., Alvino D.M., Hunter E., Allen S.A., Walker B.D. Lack of detectable HIV-1-specific CD8(+) T cell responses in Zambian HIV-1-exposed seronegative partners of HIV-1-positive individuals. J. Infect. Dis. 2011;203:258–262. - PMC - PubMed
-
- Aguilar-Jimenez W., Zapata W., Rugeles M.T. Antiviral molecules correlate with vitamin D pathway genes and are associated with natural resistance to HIV-1 infection. Microbes Infect. 2016;18:510–516. - PubMed
-
- Alimonti J.B., Kimani J., Matu L., Wachihi C., Kaul R., Plummer F.A., Fowke K.R. Characterization of CD8 T-cell responses in HIV-1-exposed seronegative commercial sex workers from Nairobi, Kenya. Immunol. Cell Biol. 2006;84:482–485. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
