

Cost-effectiveness of lobectomy versus genetic testing (Afirma®) for indeterminate thyroid nodules: Considering the costs of surveillance
- PMID: 29128178
- PMCID: PMC5736452
- DOI: 10.1016/j.surg.2017.10.004
Cost-effectiveness of lobectomy versus genetic testing (Afirma®) for indeterminate thyroid nodules: Considering the costs of surveillance
Abstract
Background: We evaluated whether diagnostic thyroidectomy for indeterminate thyroid nodules would be more cost-effective than genetic testing after including the costs of long-term surveillance.
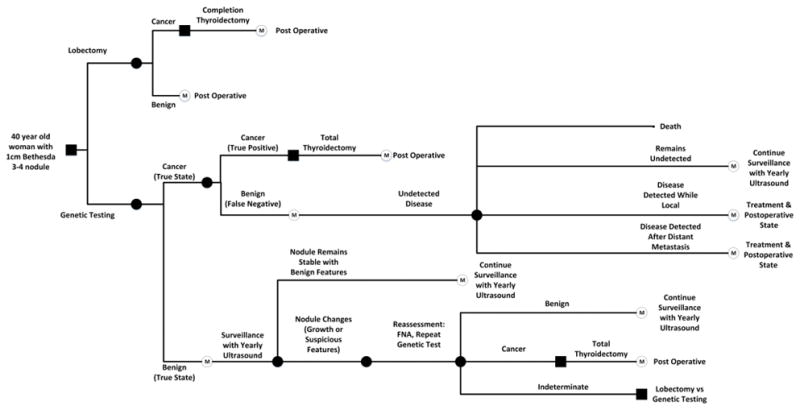
Methods: We used a Markov decision model to estimate the cost-effectiveness of thyroid lobectomy versus genetic testing (Afirma®) for evaluation of indeterminate (Bethesda 3-4) thyroid nodules. The base case was a 40-year-old woman with a 1-cm indeterminate nodule. Probabilities and estimates of utilities were obtained from the literature. Cost estimates were based on Medicare reimbursements with a 3% discount rate for costs and quality-adjusted life-years.
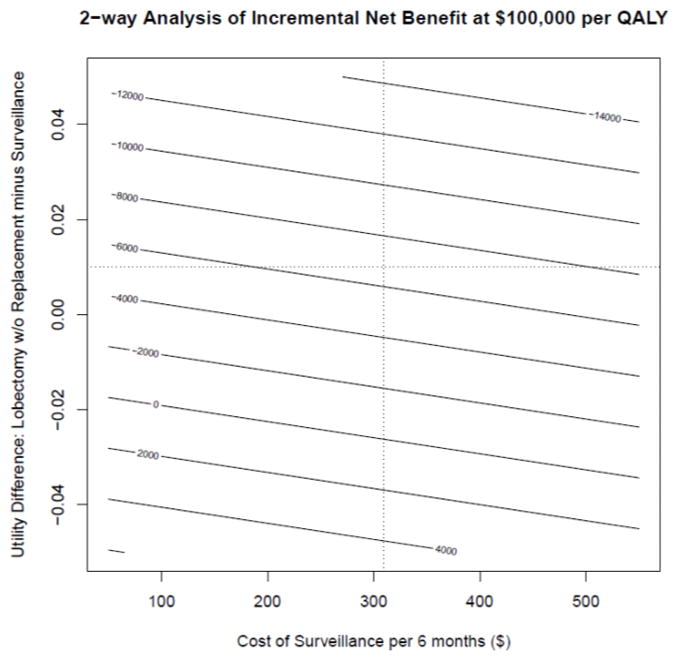
Results: During a 5-year period after the diagnosis of indeterminate thyroid nodules, lobectomy was less costly and more effective than Afirma® (lobectomy: $6,100; 4.50 quality-adjusted life- years vs Afirma®: $9,400; 4.47 quality-adjusted life-years). Only in 253 of 10,000 simulations (2.5%) did Afirma® show a net benefit at a cost-effectiveness threshold of $100,000 per quality- adjusted life-years. There was only a 0.3% probability of Afirma® being cost saving and a 14.9% probability of improving quality-adjusted life-years.
Conclusions: Our base case estimate suggests that diagnostic lobectomy dominates genetic testing as a strategy for ruling out malignancy of indeterminate thyroid nodules. These results, however, were highly sensitive to estimates of utilities after lobectomy and living under surveillance after Afirma®.
Published by Elsevier Inc.
Figures

Comment in
-
Discussion.Surgery. 2018 Jan;163(1):95-96. doi: 10.1016/j.surg.2017.10.007. Epub 2017 Nov 8. Surgery. 2018. PMID: 29128186 No abstract available.
Similar articles
-
Molecular Testing Versus Diagnostic Lobectomy in Bethesda III/IV Thyroid Nodules: A Cost-Effectiveness Analysis.Thyroid. 2019 Sep;29(9):1237-1243. doi: 10.1089/thy.2018.0779. Thyroid. 2019. PMID: 31407625 Free PMC article.
-
Cost-Effectiveness of Diagnostic Lobectomy Versus Observation for Thyroid Nodules >4 cm.Thyroid. 2016 Feb;26(2):271-9. doi: 10.1089/thy.2015.0300. Epub 2016 Jan 22. Thyroid. 2016. PMID: 26715288
-
Cost analysis of reflexive versus selective molecular testing for indeterminate thyroid nodules.Surgery. 2022 Jan;171(1):147-154. doi: 10.1016/j.surg.2021.04.050. Epub 2021 Jul 17. Surgery. 2022. PMID: 34284895
-
A Systematic Review of the Methods of Diagnostic Accuracy Studies of the Afirma Gene Expression Classifier.Thyroid. 2017 Oct;27(10):1215-1222. doi: 10.1089/thy.2016.0656. Epub 2017 Aug 17. Thyroid. 2017. PMID: 28741442 Review.
-
Long-Term Outcomes of Thyroid Nodule AFIRMA GEC Testing and Literature Review: An Institutional Experience.Otolaryngol Head Neck Surg. 2020 May;162(5):634-640. doi: 10.1177/0194599820911718. Epub 2020 Mar 17. Otolaryngol Head Neck Surg. 2020. PMID: 32182188 Review.
Cited by
-
Is There a Role for Molecular Testing for Low-Risk Differentiated Thyroid Cancer? A Cost-Effectiveness Analysis.Cancers (Basel). 2023 Jan 27;15(3):786. doi: 10.3390/cancers15030786. Cancers (Basel). 2023. PMID: 36765745 Free PMC article.
-
The Diagnostic Performance of Afirma Gene Expression Classifier for the Indeterminate Thyroid Nodules: A Meta-Analysis.Biomed Res Int. 2019 Aug 20;2019:7150527. doi: 10.1155/2019/7150527. eCollection 2019. Biomed Res Int. 2019. PMID: 31531363 Free PMC article. Review.
-
FDG-PET/CT in indeterminate thyroid nodules: cost-utility analysis alongside a randomised controlled trial.Eur J Nucl Med Mol Imaging. 2022 Aug;49(10):3452-3469. doi: 10.1007/s00259-022-05794-w. Epub 2022 Apr 18. Eur J Nucl Med Mol Imaging. 2022. PMID: 35435497 Free PMC article. Clinical Trial.
-
Recent Advances in the Surgical Management of Thyroid Cancer.Curr Oncol. 2023 May 5;30(5):4787-4804. doi: 10.3390/curroncol30050361. Curr Oncol. 2023. PMID: 37232819 Free PMC article. Review.
-
Deep-Learning-Based Screening and Ancillary Testing for Thyroid Cytopathology.Am J Pathol. 2023 Sep;193(9):1185-1194. doi: 10.1016/j.ajpath.2023.05.011. Am J Pathol. 2023. PMID: 37611969 Free PMC article.
References
-
- Mortensen JD, Woolner LB, Bennett WA. Gross and microscopic findings in clinically normal thyroid glands. J Clin Endocrinol Metab. 1955;15(10):1270–1280. - PubMed
-
- Yassa L, Cibas ES, Benson CB, et al. Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer. 2007;111(6):508–516. - PubMed
-
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133. - PMC - PubMed
-
- Alexander EK, Kennedy GC, Baloch ZW, et al. Preoperative diagnosis of benign thyroid nodules with indeterminate cytology. N Engl J Med. 2012;367(8):705–715. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
