

Model projections on the impact of HCV treatment in the prevention of HCV transmission among people who inject drugs in Europe
- PMID: 29080808
- PMCID: PMC5841161
- DOI: 10.1016/j.jhep.2017.10.010
Model projections on the impact of HCV treatment in the prevention of HCV transmission among people who inject drugs in Europe
Abstract
Background & aims: Prevention of hepatitis C virus (HCV) transmission among people who inject drugs (PWID) is critical for eliminating HCV in Europe. We estimated the impact of current and scaled-up HCV treatment with and without scaling up opioid substitution therapy (OST) and needle and syringe programmes (NSPs) across Europe over the next 10 years.
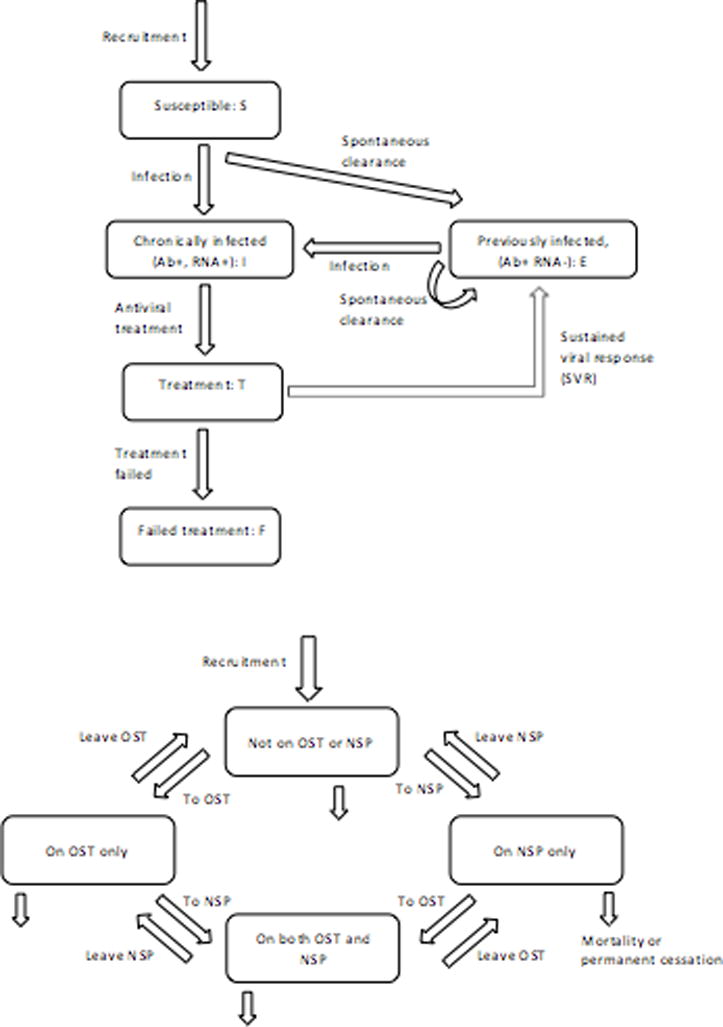
Methods: We collected data on PWID HCV treatment rates, PWID prevalence, HCV prevalence, OST, and NSP coverage from 11 European settings. We parameterised an HCV transmission model to setting-specific data that project chronic HCV prevalence and incidence among PWID.
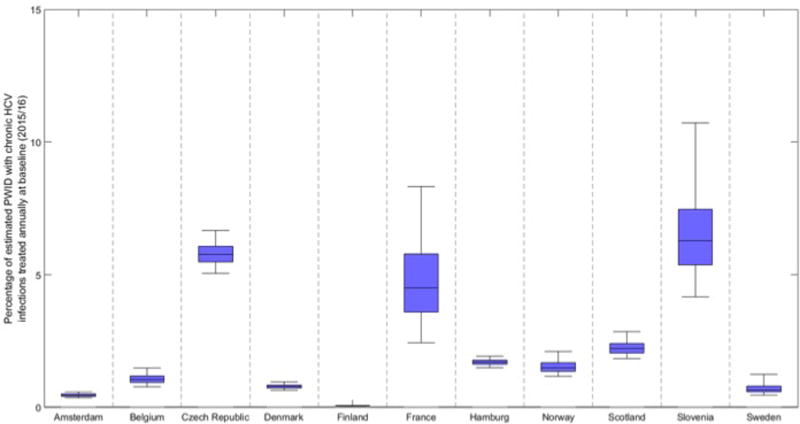
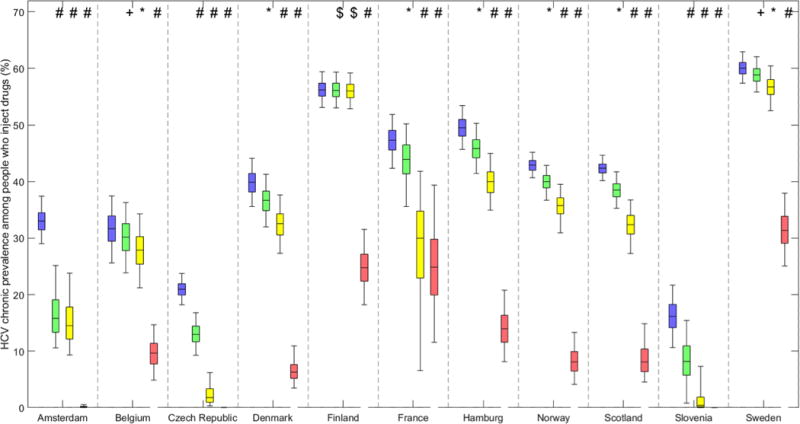
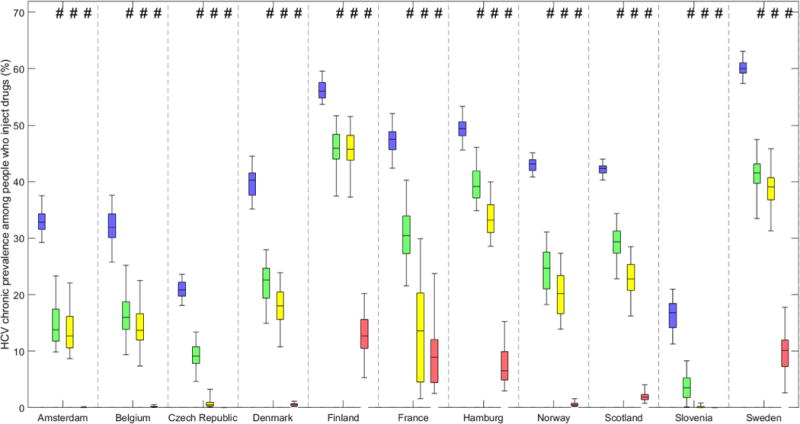
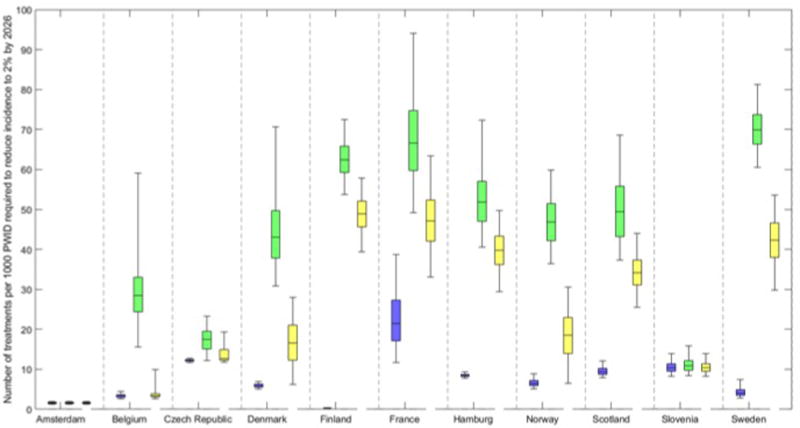
Results: At baseline, chronic HCV prevalence varied from <25% (Slovenia/Czech Republic) to >55% (Finland/Sweden), and <2% (Amsterdam/Hamburg/Norway/Denmark/Sweden) to 5% (Slovenia/Czech Republic) of chronically infected PWID were treated annually. The current treatment rates using new direct-acting antivirals (DAAs) may achieve observable reductions in chronic prevalence (38-63%) in 10 years in Czech Republic, Slovenia, and Amsterdam. Doubling the HCV treatment rates will reduce prevalence in other sites (12-24%; Belgium/Denmark/Hamburg/Norway/Scotland), but is unlikely to reduce prevalence in Sweden and Finland. Scaling-up OST and NSP to 80% coverage with current treatment rates using DAAs could achieve observable reductions in HCV prevalence (18-79%) in all sites. Using DAAs, Slovenia and Amsterdam are projected to reduce incidence to 2 per 100 person years or less in 10 years. Moderate to substantial increases in the current treatment rates are required to achieve the same impact elsewhere, from 1.4 to 3 times (Czech Republic and France), 5-17 times (France, Scotland, Hamburg, Norway, Denmark, Belgium, and Sweden), to 200 times (Finland). Scaling-up OST and NSP coverage to 80% in all sites reduces treatment scale-up needed by 20-80%.
Conclusions: The scale-up of HCV treatment and other interventions is needed in most settings to minimise HCV transmission among PWID in Europe.
Lay summary: Measuring the amount of HCV in the population of PWID is uncertain. To reduce HCV infection to minimal levels in Europe will require scale-up of both HCV treatment and other interventions that reduce injecting risk (especially OST and provision of sterile injecting equipment).
Keywords: Direct-acting antivirals; Hepatitis C; Opioid substitution therapy; PWID.
Copyright © 2017 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Achieving hepatitis C elimination in Europe - To treatment scale-up and beyond.J Hepatol. 2018 Mar;68(3):383-385. doi: 10.1016/j.jhep.2017.12.004. Epub 2017 Dec 9. J Hepatol. 2018. PMID: 29233629 No abstract available.
Similar articles
-
Modelling the impact of a national scale-up of interventions on hepatitis C virus transmission among people who inject drugs in Scotland.Addiction. 2018 Nov;113(11):2118-2131. doi: 10.1111/add.14267. Epub 2018 Jul 10. Addiction. 2018. PMID: 29781207 Free PMC article.
-
Scaling-up HCV prevention and treatment interventions in rural United States-model projections for tackling an increasing epidemic.Addiction. 2018 Jan;113(1):173-182. doi: 10.1111/add.13948. Epub 2017 Sep 20. Addiction. 2018. PMID: 28734093 Free PMC article.
-
Combination interventions to prevent HCV transmission among people who inject drugs: modeling the impact of antiviral treatment, needle and syringe programs, and opiate substitution therapy.Clin Infect Dis. 2013 Aug;57 Suppl 2(Suppl 2):S39-45. doi: 10.1093/cid/cit296. Clin Infect Dis. 2013. PMID: 23884064 Free PMC article.
-
Needle syringe programmes and opioid substitution therapy for preventing hepatitis C transmission in people who inject drugs.Cochrane Database Syst Rev. 2017 Sep 18;9(9):CD012021. doi: 10.1002/14651858.CD012021.pub2. Cochrane Database Syst Rev. 2017. PMID: 28922449 Free PMC article. Review.
-
Global, regional, and country-level coverage of interventions to prevent and manage HIV and hepatitis C among people who inject drugs: a systematic review.Lancet Glob Health. 2017 Dec;5(12):e1208-e1220. doi: 10.1016/S2214-109X(17)30373-X. Epub 2017 Oct 23. Lancet Glob Health. 2017. PMID: 29074410 Free PMC article. Review.
Cited by
-
How the rural risk environment underpins hepatitis C risk: Qualitative findings from rural southern Illinois, United States.Int J Drug Policy. 2023 Feb;112:103930. doi: 10.1016/j.drugpo.2022.103930. Epub 2023 Jan 13. Int J Drug Policy. 2023. PMID: 36641816 Free PMC article.
-
Nurse case management to improve the hepatitis C care continuum in HIV co-infection: Results of a randomized controlled trial.J Viral Hepat. 2020 Apr;27(4):376-386. doi: 10.1111/jvh.13241. Epub 2019 Dec 9. J Viral Hepat. 2020. PMID: 31750598 Free PMC article. Clinical Trial.
-
Prevalence, risk factors, treatment uptake and treatment outcome of hepatitis C virus in people who inject drugs at the needle and syringe program in Uppsala, Sweden.Harm Reduct J. 2023 Jun 16;20(1):77. doi: 10.1186/s12954-023-00806-w. Harm Reduct J. 2023. PMID: 37328868 Free PMC article.
-
Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: a multistage systematic review.Lancet Glob Health. 2017 Dec;5(12):e1192-e1207. doi: 10.1016/S2214-109X(17)30375-3. Epub 2017 Oct 23. Lancet Glob Health. 2017. PMID: 29074409 Free PMC article. Review.
-
An Increase in the Prevalence of Clinically Relevant Resistance-Associated Substitutions in Four Direct-Acting Antiviral Regimens: A Study Using GenBank HCV Sequences.Pathogens. 2024 Aug 9;13(8):674. doi: 10.3390/pathogens13080674. Pathogens. 2024. PMID: 39204274 Free PMC article.
References
-
- Williams R, et al. Addressing liver disease in the UK: a blueprint for attaining excellence in health care and reducing premature mortality from lifestyle issues of excess consumption of alcohol, obesity, and viral hepatitis. Lancet. 2014;384(9958):1953–97. - PubMed
-
- Ly KN, et al. The increasing burden of mortality from viral hepatitis in the United States between 1999 and 2007. Annals of internal medicine. 2012;156(4):271–278. - PubMed
-
- Cowie B, Allard N, MacLachlan J. O86 EUROPEAN RESPONSES IN FOCUS: COMPARING VIRAL HEPATITIS AND HIV RELATED DEATHS IN EUROPE 1990–2010 IN THE GLOBAL BURDEN OF DISEASE STUDY 2010. Journal of Hepatology. 2014;1(60):S35–S36.
-
- ECDC and EMCDDA. Prevention and control of infectious diseases among people who inject drugs. Stockholm: ECDC; 2011. pp. 4–5.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
